Bowel Incontinence
Bowel incontinence, also known as fecal incontinence, accidental bowel leakage (ABL), fecal leakage, and stool soiling, is the involuntary loss of stool or the inability to control bowel movements. Many people experience bowel incontinence, the inability to control bowel movements that causes involuntary stool leakage; you should understand common causes, symptoms, and safe natural treatment approaches to manage it effectively.
Key Takeaways:
- Bowel incontinence is the involuntary loss of stool, ranging from occasional leakage to complete loss, and it affects people of all ages, with higher rates in older adults and those with neurologic disease.
- Common causes include pelvic floor or sphincter muscle damage (childbirth, surgery, colon resection), nerve injury from diabetes or multiple sclerosis, radiation therapy, chronic diarrhea or constipation with overflow, and episodes triggered by coughing when pelvic support is weak.
- Medications that can cause or worsen bowel incontinence include laxatives, antibiotics (through antibiotic-associated diarrhea), some diabetes drugs (e.g., metformin or GLP-1 agonists), magnesium-containing antacids, and opioids (which may cause overflow incontinence via constipation).
- Common signs include sudden urgency, not being able to get to the bathroom in time, passive soiling (even while sleeping), changes in stool consistency, and social or emotional effects from leaks that happen without warning.
- First-line management focuses on conservative measures, such as changing the diet and fluid intake, scheduling bathroom breaks and bowel retraining, using anti-diarrheal medications when needed, doing pelvic floor muscle training (Kegel exercises) and biofeedback, and using absorbent products for protection.
- Natural or nonpharmacologic approaches with some evidence include soluble fiber supplements (psyllium), pelvic floor rehabilitation, timed evacuation, probiotics (limited evidence), weight loss, and acupuncture (limited and variable evidence).
- If the problem is severe or doesn’t get better, you should see a specialist; more advanced treatments can include injections to bulk up the area, repairing the sphincter, stimulating the sacral nerve, or surgery for certain patients, while treatment should also focus on the root causes like nerve issues or damage
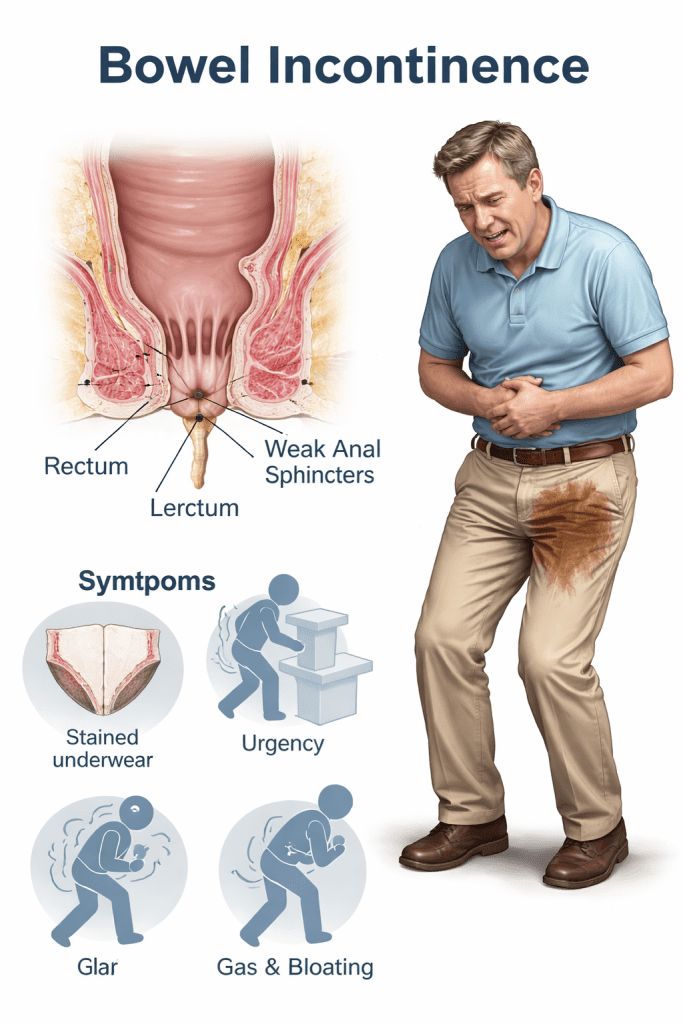
Clinical Symptoms and Classification of Bowel Incontinence
Symptoms you notice often include sudden urgency, unexpected soiling, and changes in bowel pattern; documenting bowel incontinence symptoms helps you and your clinician classify severity and triggers.
Muscle weakness around the anal sphincter or pudendal nerve injury can explain episodes where you sense no urge before leakage, a pattern consistent with passive bowel incontinence seen in clinical reports.
Frequency of events, stool consistency, and timing—including occurrences of bowel incontinence during sleep—will guide you toward categories like urge, passive, or nocturnal incontinence for targeted treatment planning.
Identifying primary physical indicators
Identifying the physical signs you can observe means tracking leakage amount, presence of mucus or blood, and any associated pain to clarify which bowel incontinence symptoms match your experience.
Pelvic floor tone was assessed during the exam, and findings such as soiling without prior awareness suggest passive bowel incontinence, which may not be felt until after leakage has occurred.
Sensation changes, including reduced rectal sensation or decreased awareness of stool, should be recorded by you and discussed with a specialist to separate sensory loss from motor dysfunction.
Distinguishing between passive and nocturnal episodes
Distinguishing passive from nocturnal episodes requires you to note whether leakage happens while awake without urge or specifically during sleep when you are unaware, which classifies many cases as bowel incontinence during sleep.
Passive events often occur with no warning and are linked to impaired sphincter closure; you will report soiling on waking or during light activity rather than after urgency.
Nighttime leakage that you discover upon waking is reported as bowel incontinence during sleep and may prompt evaluation for sleep-related bowel emptying, nocturnal diarrhea, or medication effects that you should track.
Additional details you should record include timing, mattress contamination, and any correlating medications or nocturnal diarrhea to help separate passive bowel incontinence from bowel incontinence during sleep and plan management.
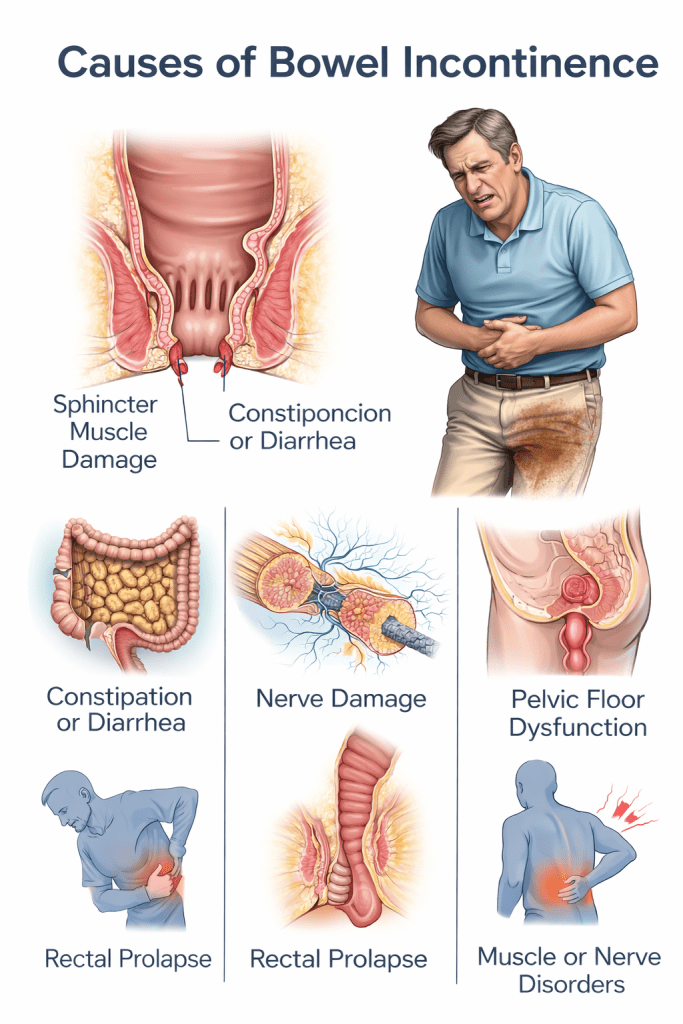
Primary Medical Causes and External Triggers of Bowel Incontinence
You will encounter a range of causes of bowel incontinence, from nerve damage and muscle weakness to stool consistency changes; knowing that lets you target treatment choices. You should note that pelvic floor injury, childbirth trauma, and neurologic disorders frequently appear on lists of causes of bowel incontinence in clinical reviews. You can track symptoms and triggers to share with clinicians so evaluation addresses the specific mechanism affecting your continence.
Chronic conditions often amplify leakage episodes; you may see small-volume urgency or passive seepage depending on the underlying pathology. Chronic bowel dysfunction can stem from metabolic disease, neurological decline, or repeated insult to the anorectal complex, and documenting frequency helps guide conservative measures. You should keep a diary of episodes, stool form, and precipitating events to help narrow the differential.
Coughing causing bowel incontinence is a common external trigger when increased intra-abdominal pressure meets weakened sphincter or pelvic floor support, so coughing fits and chronic cough deserve attention. Cough-induced leaks often present as stress-like incontinence of flatus or liquid stool rather than full evacuation. You can reduce episodes by addressing cough etiologies and strengthening pelvic support alongside medical care.
Chronic health conditions, including MS and Diabetes
When you live with MS and bowel incontinence, demyelination disrupts anorectal reflexes and can produce constipation that alternates with incontinence, so you must report patterns to your neurologist. When clinicians evaluate ms and bowel incontinence, they often test anorectal sensation and transit time to tailor bowel regimens. Coordinating neurology and gastroenterology care increases the likelihood of symptom control with targeted therapies.
If you have diabetes, bowel incontinence, peripheral neuropathy, and autonomic dysfunction, impaired sphincter control and colonic motility commonly produce mixed constipation and overflow incontinence. Poor glycemic control is more likely to affect stool consistency and sensation, so improving glucose management is beneficial. If needed, you can use timed bowel programs, osmotic laxatives, or enemas under guidance to reduce episodes.
Diabetes and MS often coexist with other contributors, requiring combined approaches you can implement at home and in the clinic. Diabetes incontinence bowel symptoms may improve with structured dietary fiber, hydration, and medication adjustments you and your provider agree on. MS and bowel incontinence management frequently involves scheduled evacuation, biofeedback when feasible, and pelvic floor therapy coordinated by your care team.
Impact of surgical procedures and radiation therapy
After pelvic surgery you may notice altered bowel habits because surgical trauma or nerve injury can reduce sphincter strength, and you should report any new leakage following procedures. After colon resection patients commonly describe changed stool frequency and consistency that can precipitate leakage; bowel incontinence after colon resection is a recognized postoperative complication. After you document the timing and characteristics of incontinence, targeted rehabilitation and dietary adjustments can be initiated.
Radiation exposure to the pelvis can cause progressive fibrosis and mucosal damage leading to bowel incontinence due to radiation, often appearing months to years after treatment and featuring urgency and loose stool. Radiation-induced effects may be persistent; you should inform your oncologist about urgency, mucus, or bleeding that accompanies incontinence. Options for managing radiation proctitis include topical sucralfate, anti-diarrheal agents, and endoscopic therapy when indicated.
Surgical approaches that alter reservoir capacity or disrupt innervation—such as low anterior resection—frequently change stool transit and continence, so you should expect and prepare for postoperative bowel changes. Surgical teams commonly counsel patients that bowel urgency and incontinence are possible and that graded rehabilitation, pelvic floor exercises, and medical therapies can reduce impact. Surgical history always informs the next steps in your continence plan.
Bowel incontinence after colon resection may respond to antidiarrheal medications like loperamide, dietary soluble fiber, and pelvic physiotherapy; you can begin early with clinician oversight to improve outcomes. Bowel incontinence after colon resection often shows similar patterns to low anterior resection syndrome, and improving stool consistency along with pelvic floor exercises can lead to noticeable benefits for many patients.
Influence of pharmacological treatments and physical strain
Medications that can cause bowel incontinence include laxatives, magnesium-containing antacids, certain antibiotics, cholinergic agents, and some antihypertensives, so you should review prescriptions whenever incontinence emerges. Medications that can cause bowel incontinence may alter stool consistency or gut motility; you can work with prescribers to adjust dosing or switch agents. Medication reviews are a straightforward first step you can request.
Certain psychotropic drugs and diabetes medications also affect bowel function, and you should be aware that side effects can mimic primary bowel disorders. Certain drug-induced diarrhea or fecal urgency responds to dose modification or substitution, and documenting timing relative to medication changes helps clinicians identify culprits. Certain nonprescription remedies and supplements deserve the same scrutiny when symptoms start.
Straining and heavy lifting increase intra-abdominal pressure and can precipitate coughing causing bowel incontinence or stress-related leakage when pelvic support is compromised, so you should modify activities and learn safe lifting techniques. Straining during bowel movements—often from constipation—can further weaken pelvic structures; hence, treating constipation reduces mechanical stress you place on your sphincter. Straining reduction is a practical element of comprehensive conservative care.
Physical factors combine with drugs to create multifactorial risk, and you should pursue a coordinated review of your medications, occupational activities, and bowel habits to identify modifiable triggers. Physical assessment, medication reconciliation, and targeted pelvic floor training you engage in often decrease episode frequency and improve quality of life.
Natural Treatment Protocols and Management Strategies for Bowel Incontinence
Physical therapy and pelvic floor strengthening
You will find that the most common baseline treatment for bowel incontinence starts with targeted pelvic floor assessment and a tailored program, because treatment for bowel incontinence often combines strength training, coordination drills, and lifestyle changes to reduce leakage. Can bowel incontinence be corrected? Often, yes, particularly when you follow an individualized plan from a pelvic floor physiotherapist over 8–12 weeks with regular home practice and symptom tracking.

A clinician should teach and progress Kegel exercises for bowel incontinence. So you perform 8–12 slow holds of 3–10 seconds and 10 quick contractions, repeated two to three times daily, focusing on squeezing inward and upward without bearing down. You should pair these with expiratory control and posture adjustments to improve anorectal closure and reduce urgency-related accidents.
Clinical biofeedback and electrical stimulation are adjuncts that teach you to sense and control sphincter responses, with many programs reporting measurable improvement in fecal urgency and soiling after structured sessions. You must communicate goals, measure outcomes, and reassess continence scores so the plan adapts as you strengthen pelvic support.
Holistic interventions and acupuncture for bowel incontinence
Acupuncture for bowel incontinence can serve as a complementary approach when you ask. How do you stop bowel incontinence naturally? Some clinics use neuromodulatory input alongside physiotherapy and diet changes to reduce urgency and frequency. You should consider sessions two times weekly initially, then tapering based on symptomatic response and practitioner guidance.
Herbal and nutritional strategies support stool consistency, which answers How to stop bowel incontinence naturally by using soluble fiber like psyllium to target stool form and probiotics to rebalance gut flora: you should consult a practitioner to select strains and doses that fit your pattern of incontinence. You will monitor effects and adjust intake over weeks rather than days.
Mind-body techniques such as diaphragmatic breathing, pelvic relaxation, and guided imagery can reduce sensory urgency and assist in retraining rectal sensation, answering What can be done for bowel incontinence? by lowering stress-related triggers and improving your control during high-risk situations. You should practice these skills daily to augment physical therapy gains.
Studies show that acupuncture for bowel incontinence can help reduce symptoms when used alongside standard treatment, so consider it as an additional option that might help you see improvements while you keep doing Kegel exercises and behavioral training.
Acupuncture for Bowel Incontinence
Acupuncture is a promising, safe, and potentially effective complementary therapy for managing fecal incontinence, often improving anal sphincter tone, nerve function, and quality of life. Studies show significant improvement in continence scores, with some patients reporting no symptoms after 10-12 weeks of treatment.
How Acupuncture Helps Bowel Incontinence
-
- Improves Muscle Tone: It helps strengthen the striated pelvic muscles, which are vital to preserving continence.
- Neuromodulation: It can adjust how the rectum and anus work, much like sacral nerve stimulation does, enhancing nerve activity in the lower back and belly
- Regulates Bowel Habits:
It can help regulate gastrointestinal motility, aiding in both cases of chronic diarrhea and constipation-related overflow.
-
Reduces Symptoms: Studies suggest acupuncture can reduce the frequency of involuntary leakage.
Key Details regarding Treatment
- Duration: Positive results have been reported after a course of treatment, such as one session per week for 10–12 weeks.
- Effectiveness: Although numerous studies suggest its efficacy, some evidence derives from smaller studies, necessitating additional high-quality, randomized controlled trials.
- Techniques: Specialized techniques, such as electroacupuncture, may offer specific benefits for neurogenic fecal incontinence by enhancing anal sphincter muscle activity.
Hypnotherapy for Bowel Incontinence

- Targeting the Brain-Gut Axis: It reduces overactivity in the gut by calming the miscommunication between the brain and the digestive system, which is a key contributor to urgency and accidents.
- Modulating Gut Sensations: It helps reduce abdominal pain, visceral hypersensitivity, and diarrhea, reducing the urgency that often leads to incontinence.
- Mental Control Techniques: It teaches patients to gain control over involuntary physiological mechanisms of the bowel, often using visualizations like a “calm, relaxed, or perfectly functioning” gut.
According to data from the UK published in the American Journal of Gastroenterology, hypnosis therapy seems to be a successful treatment for bowel incontinence.
BOWEL INCONTINENCE is characterized by a range of functional symptoms, such as episodes of diarrhea, constipation, bloating, and stomach discomfort. It is more common in women than in men, and its etiology is unknown.
Previous research has demonstrated that hypnotherapy is an effective treatment for BOWEL INCONTINENCE, even though it is not a psychiatric condition. Six therapists work in a hypnotherapy unit established by the UK’s National Health Service. This paper assesses the efficacy of the treatment for the first 250 patients in the unit. There was no control group, and it was not a clinical trial. It is merely a questionnaire-based audit of the healthcare services rendered.
Over the course of three months, the participants received twelve hypnotherapy sessions and practiced the skills on an audiotape in between. Following hypnotherapy, patients reported both an overall improvement in their condition and improvements in particular areas, such as the frequency and intensity of their discomfort, bloating, discontent with their bowel habits, and the degree to which BOWEL INCONTINENCE interfered with their daily lives.
In fact, following hypnotherapy, over three-quarters (78%) of the study participants reported changes in their bowel pattern, or stool frequency and consistency. For the remaining people, there was either no change (13%) or a minor decline (9%).
Following hypnotherapy, the patients’ reported extracolonic symptoms—such as tiredness, body aches, backaches, and urine symptoms—improved. According to reports, the therapy also lessened the patients’ anxiety and sadness and enhanced their quality of life.
However, the results of the study indicate that women appeared to benefit more from the treatment than males did. Women complained of more severe bloating at the beginning of the trial and assessed their BOWEL INCONTINENCE and non-colon-related symptoms as more severe than did men. However, the women evaluated their non-colon-related symptoms and BOWEL INCONTINENCE lower than the men did following hypnosis.
Men with diarrhea may have improved less than women, especially in terms of how much their BOWEL INCONTINENCE affected their lives and how unhappy they were with their bowel habits, which may have contributed to the score disparity.
“This study clearly demonstrates that hypnotherapy remains an extremely effective treatment for bowel incontinence and should prove more cost-effective as new, more expensive drugs come on the market,” said lead author Dr. Wendy M. Gonsalkorale. Based on earlier research, the authors of the article are certain that hypnotherapy will have an effect.
- High Success Rates: Studies show GDH reduces symptom severity in up to 71% of refractory patients, making it a powerful tool when traditional methods fail.
- Treatment Protocol: Usually, there are 4 to 12 sessions with a qualified therapist. The “Manchester Protocol,” which includes education and daily practice with audio recordings, is often used.
- Short and Long-Term Results: Research suggests improvements can last for years after treatment ends.
- Digital Options: App-based programs, such as Nerva, now offer guided gut-directed hypnotherapy (15-minute daily sessions) as an accessible alternative to in-person therapy.
- Not a Quick Fix: It requires commitment, often involving daily practice for 6-8 weeks.
- Best for Functionality: It is most effective for functional bowel issues rather than conditions caused solely by structural damage.
- Expert Care: For the best results, it is recommended to see a professional trained in gut-directed hypnotherapy.
Homeopathic Treatment for Bowel Incontinence

Commonly Used Homeopathic Remedies
- Causticum: Often recommended for involuntary stool that occurs while passing flatus, coughing, or sneezing. It is also used when there is a sensation of paralysis in the rectum.
- Aloe socotrina (Aloe): Used for involuntary stool, especially when there is a constant, urgent need to pass stool and a feeling of weakness in the sphincter.
- Podophyllum: Indicated for diarrhea-related incontinence, particularly when stool is sudden, profuse, and, in some cases, painless.
- Nux vomica: Often used when incontinence is related to constipation with frequent, ineffectual urges (“never-get-done” feeling).
- Hyoscyamus: Sometimes used when there is a sudden, uncontrollable urge to pass stool.
- Silicea (Silica): Indicated when stool is firm, dry, and accompanied by significant straining.
- Calcarea carbonica: Considered when there is significant anxiety associated with bowel movements and the stools are large.
Supporting Natural Measures
- Pelvic Floor Exercises (Kegels): These are recommended to strengthen the muscles that control the bowels.
- Dietary Adjustments: Increasing dietary fiber can help make stool firmer and easier to control.
- Hygiene: Gently cleaning the anal area with water rather than soap can help prevent irritation.
Important Considerations
- Individualization: Homeopathic remedies are not universally applicable and are selected based on an individual’s complete symptom profile.
- Safety: The National Institutes of Health (NIH) states that there is much significant evidence supporting the effectiveness of homeopathy for any specific condition.
- Consult a Professional: A professional homeopath should be consulted for a customized remedy and potency (e.g., 6c is sometimes mentioned, but the dosage depends on the individual).
Behavioral modifications and corrective techniques
Dietary adjustments are the first-line steps when you ask How to manage bowel incontinence: aim for 20-30 grams of soluble fiber daily, avoid high-fat trigger meals, and limit caffeine and alcohol, which can increase urgency; you should keep a short food-and-symptom log to identify personal triggers.
Routine bowel training uses timed toileting and scheduled laxative adjustments to create predictable emptying windows so you can reduce accidents by sitting on the toilet for 10-15 minutes at set times (for example, after meals) and gradually extend intervals as control improves. You should work with a clinician to set an achievable schedule.
Pelvic biofeedback and toileting technique coaching teach you to coordinate abdominal pressure with sphincter contraction and to use corrective techniques such as gentle anterior pelvic tilt and perineal support, directly addressing What can be done for bowel incontinence? by improving evacuation mechanics and minimizing passive leakage; you should practice these cues during all toileting attempts. Monitoring symptoms with a bowel diary, Bristol Stool Chart entries, and incontinence episode counts helps you quantify progress and informs medication or device adjustments, so you should review this data with your provider every 4-6 weeks to refine the management strategy.
Final Words
So you can follow a clear summary of how to stop bowel incontinence naturally and options for managing or correcting the condition: perform pelvic floor (Kegel) exercises—three sets daily of 8–12 squeezes; practice bowel retraining with scheduled toileting every 2–3 hours; and add soluble fiber such as psyllium (5–10 g) twice a day (10–20 g/day total) to regulate stool form.
You may use biofeedback with a trained therapist to improve sphincter control and consider sacral nerve stimulation (InterStim) or sphincteroplasty when conservative care fails; discuss these options with a colorectal surgeon or gastroenterologist if symptoms persist despite 8-12 weeks of therapy.
You should keep a bowel diary, avoid triggers like caffeine and alcohol, maintain a healthy weight, and seek medical review for blood, sudden changes, or progressive symptoms so you receive targeted treatment promptly.
FAQ

Q: What is bowel incontinence and what are the common symptoms?
A: Bowel incontinence is the involuntary loss of stool or the inability to control bowel movements. Common symptoms include occasional leakage, urgency with an inability to reach a toilet, stains on underwear, repeated soiling, passive leakage without awareness, nighttime episodes, and a feeling of incomplete emptying.
Q: What are the main causes of bowel incontinence?
A: Causes include damage to the anal sphincter or pelvic floor (childbirth-related tears or surgery such as colon resection); nerve damage from diabetes, multiple sclerosis, spinal cord injury, or stroke; chronic diarrhea or loose stools; severe constipation with overflow incontinence; pelvic radiation; certain medications (laxatives, some antibiotics, and drugs that cause diarrhea); and age-related muscle weakness. Repetitive strong coughing can worsen pelvic floor weakness and trigger leakage in people with an already weakened sphincter.
Q: How does bowel incontinence differ in children and older adults, including those with dementia?
A: Children often have incontinence due to constipation with stool withholding, developmental issues, or congenital anorectal malformations. Older adults commonly develop incontinence from decreased mobility, reduced rectal sensation, pelvic muscle weakening, dementia-related loss of toileting awareness, and medications. People who are weak or have trouble thinking are more likely to have passive incontinence and nighttime episodes.
Q: What tests and medical treatments are available and can bowel incontinence be corrected?
A: Evaluation usually starts with history, physical and rectal exam, stool consistency assessment, and tests such as anorectal manometry, endoanal ultrasound, colonoscopy, and imaging when needed. Medical treatments include dietary fiber or bulking agents, antidiarrheal drugs (loperamide), bowel-regulating regimens, topical skin care, biofeedback, pelvic floor physiotherapy, sacral nerve stimulation, injectable bulking agents, sphincter repair surgery, and colostomy for refractory cases. Correction depends on cause and severity: some patients achieve full continence with conservative or surgical therapies, while others improve symptom control and quality of life.
Q: What natural and conservative approaches help manage or reduce bowel incontinence?
A: Dietary measures such as increasing soluble fiber (psyllium), avoiding trigger foods (spicy foods, caffeine, alcohol), and regulating fluid intake improve stool consistency. Scheduled toileting and a bowel program using the gastrocolic reflex after meals reduce accidents. Pelvic floor exercises and supervised biofeedback strengthen sphincter control. Weight loss, pelvic floor physiotherapy, and treating constipation or diarrhea medically are effective conservative steps. Probiotics and mindful eating may help in selected cases.
Q: How effective are Kegel exercises and acupuncture for bowel incontinence?
A: Pelvic floor exercises (Kegels) improve muscle strength and endurance and are effective when performed correctly and consistently, especially with guidance from a pelvic floor therapist and biofeedback; typical programs involve multiple daily sets over several months. Acupuncture has limited and mixed evidence; some small studies report modest symptom improvement as an adjunctive therapy, but acupuncture should not replace established treatments.
Q: What immediate steps can someone take at home during an episode and to reduce future accidents?
A: Immediate steps include cleaning and protecting the skin, using absorbent pads or underwear, changing clothes promptly, and using over-the-counter antidiarrheal medication for acute loose stools if appropriate. Preventive measures include starting a fiber supplement, establishing scheduled toileting (especially after meals), performing regular pelvic floor exercises, avoiding known dietary triggers, managing chronic diarrhea or constipation with a clinician, and seeking medical evaluation for persistent or worsening symptoms.
Treatment for bowel incontinence in Philadelphia, PA
Consider a holistic approach to treating bowel incontinence if you or a member of your family has experienced chronic bowel incontinence despite receiving unsuccessful treatment from Western physicians.
The Philadelphia Holistic Clinic is the #1 naturopathic facility in Brotherly Love. All holistic techniques, such as homeopathy, acupuncture, hypnosis, and energy healing, are available under one roof at the clinic.
Contact us at (267) 403-3085 to schedule your evaluation appointment with Dr. Tsan and discuss which holistic approach is best for you.