Thoracic Outlet Syndrome
Thoracic Outlet Syndrome arises when nerves or blood vessels are compressed at the thoracic outlet, often from congenital anomalies, trauma, poor posture, or repetitive motion; you may experience neck or shoulder pain, numbness, arm weakness, swelling, or vascular changes. Understanding neurogenic, arterial, and venous types guides management. For many, conservative and holistic approaches—targeted physical therapy, posture correction, trigger-point work, acupuncture, guided nerve blocks, and complementary remedies—can reduce your symptoms and help you avoid or delay surgery.
Key Takeaways:
- Causes: compression of neurovascular structures at the thoracic outlet by anatomical variants (cervical rib, scalene or pec minor hypertrophy), trauma, repetitive overhead activity, or poor posture.
- Types: three main forms—neurogenic (most common), venous (effort thrombosis, swelling), and arterial (ischemia, coldness, diminished pulses).
- Symptoms: upper limb pain, numbness, tingling, weakness, hand clumsiness, neck/shoulder pain; vascular cases add swelling, cyanosis, venous congestion or ischemic signs.
- Systemic effects: Thoracic Outlet Syndrome does not typically cause systemic high blood pressure or hormonal changes such as early menopause; it may alter blood flow to the affected limb but not systemic hypertension or endocrine function.
- Conservative treatments: first-line care includes physical therapy (posture correction, scalene/pectoralis stretching, and scapular stabilization), activity modification, myofascial/trigger-point therapy, and diagnostic/therapeutic nerve blocks.
- Interventional/surgical options: Botox can relieve scalene spasm but is contraindicated in pregnancy, active infection at the site, and neuromuscular junction disorders; refractory cases may require first-rib resection/scalenectomy or, rarely, spinal cord stimulation for chronic neuropathic pain.
- Holistic and adjunctive approaches: acupuncture and manual therapy may reduce pain and improve function for some patients; homeopathic remedies lack reliable evidence and should not replace evidence-based care.
Understanding Thoracic Outlet Syndrome
Definition
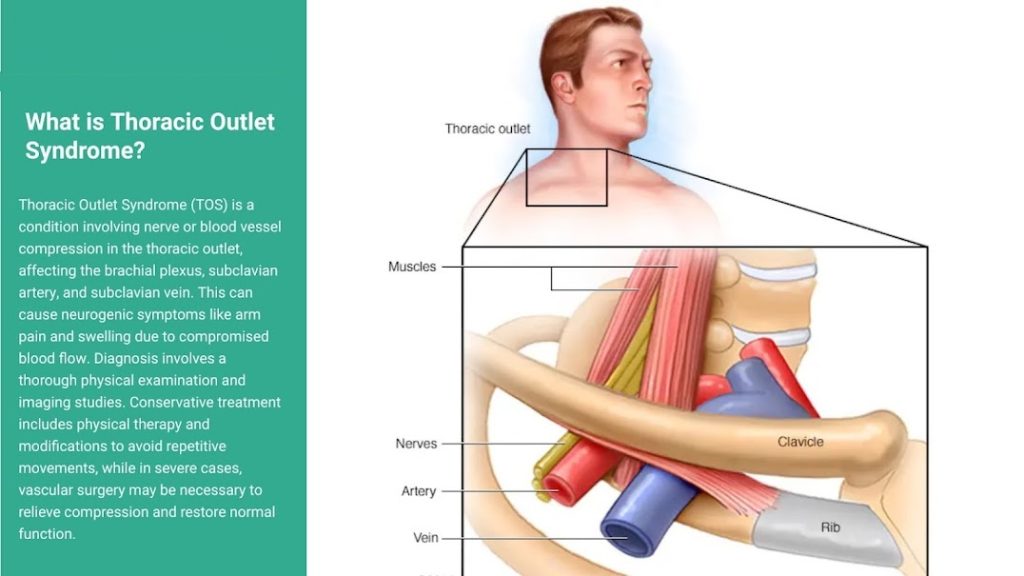
You should understand thoracic outlet syndrome (TOS) as a cluster of symptoms caused by compression of the neurovascular bundle as it exits the chest toward the arm, rather than a single, uniform disease. In practice, that means you may experience very different presentations depending on whether the brachial plexus, subclavian artery, or subclavian vein is most affected; clinically, about 90–95% of patients present with neurogenic Thoracic Outlet Syndrome, roughly 3–5% with venous Thoracic Outlet Syndrome (often Paget–Schroetter or effort thrombosis), and fewer than 1% with true arterial Thoracic Outlet Syndrome When you read case notes or studies, expect neurogenic cases to describe paresthesia, weakness, and muscle wasting patterns, whereas venous cases emphasize swelling and thrombosis, and arterial cases focus on ischemia, coldness, and distal emboli.
When you consider mechanisms, there are two overlapping explanatory frameworks clinicians use: anatomical compression and dynamic or positional compression. Anatomical causes include congenital anomalies such as a cervical rib (present in about 0.5–1% of the population), hypertrophy or fibrosis of scalene muscles, or first-rib abnormalities; dynamic causes include repetitive overhead activity, sustained poor posture, or acute trauma that narrows the scalene triangle, costoclavicular space, or subcoracoid/subpectoral space. For you this distinction matters because it directs management: static structural compression often leads to surgical discussion (for example, first-rib resection with scalenectomy), while dynamic compression is frequently addressed with targeted rehabilitation, ergonomic change, and soft-tissue work.
When you evaluate symptoms, keep the spectrum in mind. Neurogenic compression usually causes burning and numbness in the ulnar area, night pain, and noticeable weakness in the hand muscles in severe cases; venous compression often leads to sudden swelling in the arm, blue discoloration, and pain, which can be confirmed with a duplex ultrasound showing a blood clot; arterial compression may result in weak pulses, poor blood flow to the fingers, or blood clots In practical terms, you will rarely rely on a single clinical test—composite assessment, imaging (duplex, CT angiography, and MRI), and electrodiagnostics are combined to reach a working diagnosis that then shapes your treatment choices.
Anatomy of the Thoracic Outlet
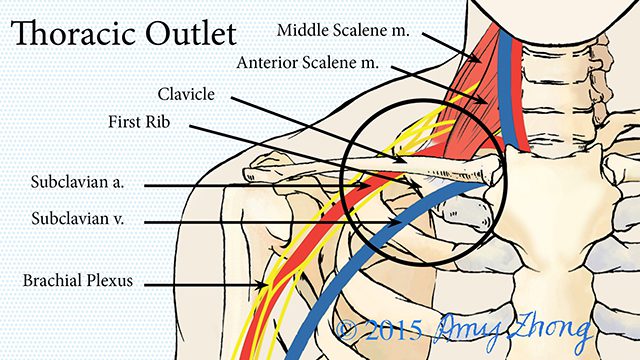
You need to visualize three anatomical tunnels through which the neurovascular structures pass to understand where compression occurs: the interscalene (or scalene) triangle, the costoclavicular space, and the subpectoral (or pectoralis minor) space. The scalene triangle is bounded by the anterior and middle scalene muscles and the first rib; it commonly compresses the lower trunks of the brachial plexus and the subclavian artery. The costoclavicular space—between the clavicle and first rib—can be narrowed by postural droop, clavicular fracture malunion, or a high-riding first rib, compressing both artery and vein. Finally, the subpectoral space under the pectoralis minor tendon is implicated in athletes and manual workers who repeatedly abduct and externally rotate the shoulder.
You should also picture the individual structures: the brachial plexus roots and trunks (C5–T1) are most susceptible to stretch and compression because of their length and branching pattern, while the subclavian vein sits anterior to the anterior scalene and is particularly vulnerable in the costoclavicular region. Clinically relevant variants include a cervical rib or long C7 transverse process that alters the scalene triangle geometry, hypertrophied anterior scalene muscle after overhead activity, and fibrous bands from the cervical rib to the first rib. Imaging reports often note these variants, as they directly impact the recommendation for surgical resection, scalenectomy, or targeted myofascial release.
You should be aware that small shifts in posture or shoulder girdle position can change cross-sectional area in these spaces by up to 30–40% during overhead work, which explains why symptoms may be intermittent and task-specific. Dynamic ultrasound and provocative tests timed with posture changes often reveal compression not apparent on static imaging, so when your clinical history reports activity-related symptoms, incorporate dynamic evaluation into diagnostic planning.
Importance of Diagnosis
You need to tell Thoracic Outlet Syndrome apart from more common conditions because the treatments are entirely unique: issues like cervical radiculopathy, rotator cuff problems, carpal tunnel syndrome, and peripheral neuropathies often look For example, a patient with C6 radiculopathy may present with lateral forearm pain and weakness similar to TOS, but an MRI of the cervical spine and specific reflex testing will direct you away from thoracic outlet interventions. Diagnostic testing—nerve conduction studies showing lower-trunk brachial plexus slowing, duplex ultrasound for venous thrombosis, CT angiography for arterial lesions, and dynamic provocative testing (Roos, Adson, Wright)—helps you stratify patients into neurogenic, venous, or arterial categories and plan conservative versus surgical strategies accordingly.
You should also consider the timing: if venous TOS is diagnosed late, it can lead to serious blood clots in the subclavian-axillary area, which can cause a risk of pulmonary embolism, while long-term pressure on nerves may cause permanent damage Data from surgical studies indicate that treating venous and arterial cases early usually leads to better chances of saving the limb and reducing symptoms, while waiting too long to treat neurogenic TOS with muscle loss results in a worse outlook for complete recovery. In clinical triage, therefore, prioritize duplex ultrasound and hematology workup for acute swelling and electrophysiology plus imaging for chronic sensory-motor patterns.
You need to integrate patient factors—occupation, athletic profile, trauma history, and anatomical variants—into your diagnostic algorithm because they change pretest probability and influence interventions. For example, a competitive swimmer or weightlifter who experiences swelling or tingling during exercise is more likely to benefit from a focused rehabilitation program that strengthens shoulder muscles and stretches the chest, while a patient with a known cervical rib and blood flow issues is more likely to be sent for a vascular surgery assessment. Applying this tailored approach reduces unnecessary surgery and improves outcomes of conservative care.
If you suspect someone has TOS, it is important to order tests in a logical sequence: start with basic vascular imaging if you think there might be issues with veins or arteries, do an EMG/NCS if nerve symptoms are the main concern, and use positional or dynamic imaging if the usual tests don’t give clear answers—this
Causes of Thoracic Outlet Syndrome
Anatomical Factors
You encounter the anatomical contributors when narrow spaces between the clavicle, first rib and scalene muscles leave little room for the brachial plexus and subclavian vessels; neurogenic TOS accounts for roughly 90–95% of cases, while venous and arterial forms constitute the remainder (venous ~3–5%, arterial ~1–2%). Structural variations such as a cervical rib (present in about 0.5–1% of the population), an elongated C7 transverse process, or an unusually high first rib can reduce the thoracic outlet cross-sectional area and convert a previously asymptomatic limb into one with paresthesia, weakness, or vascular signs. When you have one of these congenital differences, even minor muscle tightness or repetitive use can tip you into symptomatic territory.

You should pay attention to muscular anatomy as well: hypertrophy or spasm of the anterior and middle scalene muscles, or a shortened pectoralis minor, can effectively create a soft-tissue tunnel that compresses nerve or vascular structures. Athletes who perform repeated overhead motions—swimmers, pitchers, and weightlifters—commonly develop these muscle patterns over years, and imaging or dynamic EMG often shows positional narrowing of the outlet during provocative maneuvers. Imaging studies (X‑ray, CT, MRI) that identify a cervical rib or first‑rib anomaly are particularly useful when you present with arterial signs or objective ischemia.
Common anatomical variations that predispose you to compression include:
- Cervical rib or elongated C7 transverse process
- Congenital bands and fibrous slips tethering the brachial plexus
- Anomalous first rib shape or high clavicular position
The combination of a fixed bony anomaly and dynamic soft-tissue tightness is what most often converts an anatomical variant into symptomatic thoracic outlet syndrome.
Trauma and Injury
You develop post‑traumatic thoracic outlet problems after direct blunt injuries: clavicle fractures, first‑rib fractures, or sternoclavicular dislocations can change the local anatomy by callus formation or malunion, narrowing the costoclavicular or subcoracoid spaces. Whiplash from motor vehicle collisions commonly produces scalene and levator scapulae strain with subsequent fibrosis; several case series show delayed onset of paresthesia and weakness weeks to months after the initial trauma as scar tissue matures. If you’ve had thoracic or neck surgery, scar bands or postoperative edema may similarly precipitate compression.
Repeated microtrauma is another mechanism: repetitive overhead athletes or manual workers who subject the shoulder girdle to small but frequent stresses develop perineural fibrosis and muscle hypertrophy that gradually restrict the outlet. Sometimes, procedures like placing a central venous catheter or inserting a pacemaker can damage the subclavian vein, which may cause a blood clot and lead to venous thoracic outlet syndrome, also called effort thrombosis. Clinical reports document cases of Paget‑Schröetter syndrome in young athletes after vigorous exertion, linking effort and trauma to acute venous obstruction.
Vascular injuries from trauma can be dramatic: an arterial injury may present with coolness, pallor, diminished pulses, and a systolic bruit, whereas a venous injury typically produces swelling, cyanosis, and visible collateral veins; a neurogenic injury more often gives you numbness and weakness without overt color change. You may not see symptoms immediately—fibrosis and scar contracture frequently create a delayed presentation that requires a high index of suspicion after any clavicular, first‑rib or neck trauma.
More detailed clinical patterns after injury help guide your evaluation: intensity of pain, timing of onset (immediate vs. delayed), and whether swelling or ischemic signs dominate will influence whether imaging, duplex ultrasound, or referral for vascular surgery is appropriate.
Posture and Occupational Hazards
You experience thoracic outlet problems related to posture when you have a forward head position, rounded shoulders, and a curved upper back for a long time; keeping your shoulder blades pushed forward tightens the pectoralis minor muscle and stretches the muscles that stabilize the shoulder blade, which can narrow the space under the corac Many people who sit at a computer for an eight‑hour workday develop these imbalance patterns; observational studies link prolonged seated work and mobile device use with increased neck and shoulder pain that often precedes TOS symptoms. If your workstation places the monitor too low or your keyboard too far forward, the altered shoulder mechanics can become a direct contributor to nerve and vessel compression.
Occupations that force repeated arm elevation—painters, electricians, carpenters, assembly‑line workers—create a different mechanical problem by repeatedly impinging the neurovascular bundle between the clavicle and first rib. Carrying heavy loads on one side (tool belts, handbags) produces asymmetrical shoulder depression, and flight attendants or warehouse workers who repeatedly lift overhead are classically overrepresented among people who develop effort‑related venous TOS. Ergonomic assessments often reveal that simple changes in task distribution or tool use substantially reduce provocative positions.
Consistently having bad posture puts extra stress on the areas around the collarbone and shoulder, making you tire out more quickly and putting pressure on the nerves in your arm; just shortening the pectoralis minor muscle can cause many of your symptoms during tests. Physical therapy that targets scapular stabilization and lengthening of the anterior shoulder girdle often results in measurable improvements in range of motion and symptom scores, highlighting how reversible postural contributors can be.
Practical steps you can implement include ergonomic re‑evaluation of sitting posture, positioning the monitor at eye level, scheduling microbreaks every 20–30 minutes, and integrating targeted stretching and scapular stabilization exercises into your daily routine to prevent posture‑related narrowing of the outlet.
Other Contributing Factors
You should think about other factors in your body and lifestyle that don’t change your bone structure but can make compression problems more likely; conditions like Factor V Leiden and prothrombin gene mutations, along with taking estrogen, can raise the risk of blood clots and may turn minor compression into a serious issue. Diabetes and peripheral neuropathy lower the threshold at which you feel ischemic or compressive nerve symptoms, so a relatively small degree of compression can produce pronounced paresthesia and weakness in someone with metabolic neuropathy. Obesity increases mechanical load on the shoulder girdle and shifts scapular mechanics, making you more susceptible to TOS even without a bony anomaly.
Smoking and peripheral vascular disease worsen arterial reserve, which means that a mildly narrowed subclavian artery can become clinically important if your distal circulation is already compromised. Connective tissue disorders such as hypermobile Ehlers‑Danlos variants change shoulder girdle stability, producing recurrent subluxation and traction on the plexus; case series describe disproportionate rates of positional neurogenic symptoms in hypermobile patients. Pregnancy can worsen symptoms temporarily through fluid shifts, weight gain and increased anterior thoracic loading that accentuates postural imbalances.
Other modifiers to assess in your history and exam include:
- Coagulopathy or current anticoagulant/estrogen use
- Connective tissue disorder or generalized hypermobility
- Smoking, obesity, and metabolic neuropathy (e.g., diabetes)
You should interpret these factors as amplifiers—when they coexist with anatomical or occupational contributors, your risk of symptomatic thoracic outlet syndrome rises considerably.
If you have these other factors, you should also think about doing specific blood tests for blood clots if you might have them, checking for joint issues if your joints are loose, and making serious changes to your lifestyle (like quitting smoking, managing blood sugar, and controlling weight) to help your blood vessels and nerves work better.
- Order duplex ultrasound or venography sooner if you have a prothrombotic state and acute arm swelling
- Prioritize posture and strength rehabilitation when hypermobility coexists with symptomatic compression
- Coordinate with endocrine or hematology specialists when systemic contributors are identified
You will often get the best outcomes by addressing these systemic and lifestyle modifiers alongside anatomical and occupational interventions.
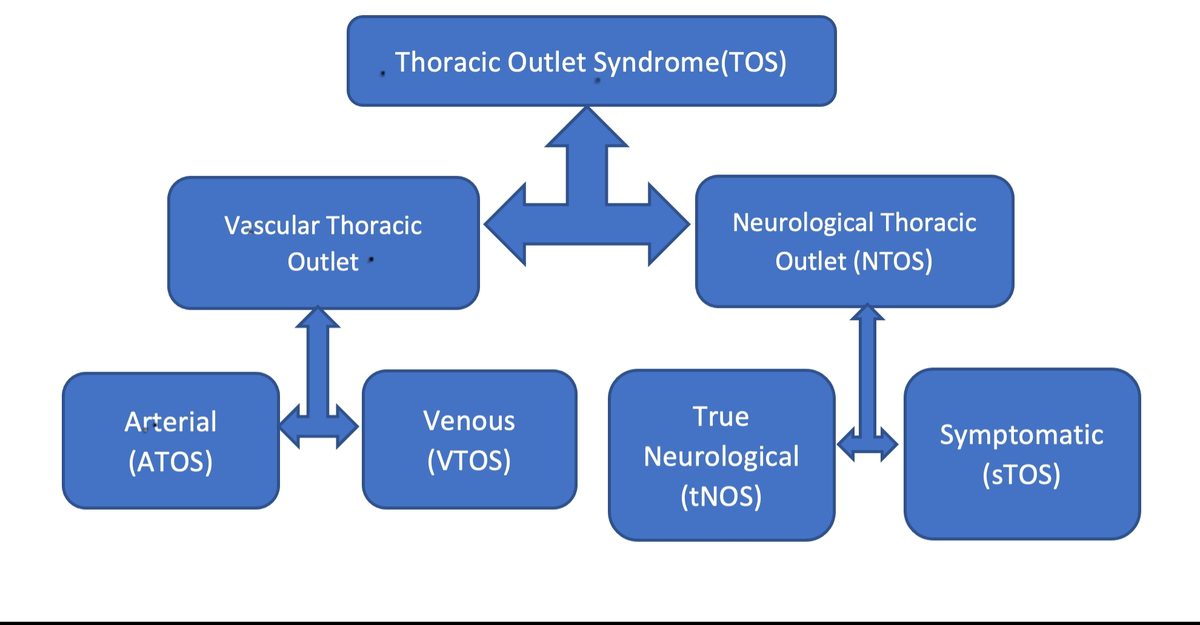
Types of Thoracic Outlet Syndrome
- Neurogenic Thoracic Outlet Syndrome—nerve compression of the brachial plexus causing pain, numbness, and weakness.
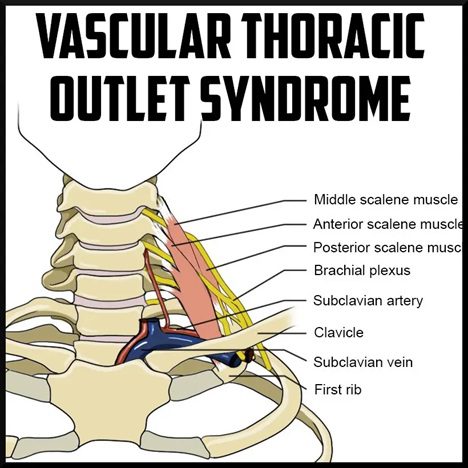
- Venous Thoracic Outlet Syndrome refers to the compression of the subclavian vein, which can result in swelling, cyanosis, and thrombosis.
- Arterial Thoracic Outlet Syndrome refers to the compression of the subclavian artery, which can lead to ischemia, aneurysm, or embolization.
| Type | Highlights |
| Neurogenic | The most common form accounts for about 90–95% of clinical presentations. The condition typically affects the brachial plexus (usually lower trunk C8–T1), causing symptoms such as pain, paresthesia, hand weakness, or intrinsic muscle wasting. The diagnosis is often clinical, with EMG/NCV providing objective confirmation in a subset of patients. Initially, patients are managed with targeted physical therapy, soft-tissue work, and selective injections. |
| Venous | Venous thrombosis, which accounts for roughly 5–10% of cases, often manifests as effort thrombosis (Paget–Schroetter) in younger, active individuals. Diagnosis typically involves duplex ultrasound and venography, and treatment typically involves thrombolysis, anticoagulation, and surgical decompression to prevent recurrence. |
| Arterial | The condition is less common, accounting for only 1-2% of cases, but it poses the highest risk for limb-threatening events—subclavian artery compression, which is often caused by a cervical rib or hypertrophic scalene. Patients typically present with pallor, coolness, diminished pulses, or distal emboli. CTA/angiography guides both surgical repair and decompression. |
| When to act | If you have progressive neurological deficit, acute swelling, loss of pulse, or signs of ischemia, you should pursue urgent vascular or surgical evaluation; multidisciplinary care (vascular surgery, neurology, and physical therapy) improves outcomes. |
Neurogenic Thoracic Outlet Syndrome
When you have neurogenic TOS, the pathology centers on mechanical irritation or compression of the brachial plexus—most commonly the lower trunk—between the anterior and middle scalene muscles, behind the clavicle, or at the retropectoralis minor space. Clinical presentations vary from intermittent paresthesia and aching to persistent neuropathic pain and objective weakness; you might notice numbness along the ulnar border of your forearm or weakness closing your hand. In epidemiologic series, the majority of patients labeled neurogenic have symptoms without definitive electrodiagnostic changes—often called disputed neurogenic TOS—while a smaller subset demonstrates clear denervation on needle EMG consistent with C8–T1 involvement.
For you, diagnostic clarity often requires combining examinations: provocative maneuvers (Adson, Roos, and costoclavicular tests), careful neurologic testing of intrinsic hand muscles, and selective use of electrodiagnostic studies. Imaging such as high-resolution ultrasound or MRI with neurography can show nerve crowding or fibrous bands in some cases, but normal imaging does not exclude symptomatic compression. Treatment is tiered: you should start with a structured conservative program emphasizing postural correction, scalene stretching, scapular stabilization, and neural gliding; clinical series report meaningful symptom reduction in many patients after 6–12 weeks of targeted therapy, though those with objective nerve injury more often require procedural intervention.
If symptoms continue even after thorough conservative treatment, you might need to consider more advanced options: these include injections into the scalene muscles (using local anesthetic with or without corticosteroids or botulinum toxin in some cases), ultrasound-guided nerve blocks for better diagnosis, or surgery to relieve pressure if there are serious issues In surgical studies, certain patients with true neurogenic TOS experience lasting relief from pain and improved strength after having the first rib and scalene muscles removed, but how well they do depends on how long they’ve had symptoms and how much nerve damage there is—longer nerve damage usually means recovery takes longer or may not You should weigh the rehabilitation timeline afterward carefully, since restoring full hand function can take months and requires coordinated postoperative physical therapy and sometimes nerve-specific rehabilitation techniques.
Arterial Thoracic Outlet Syndrome
Arterial TOS arises when the subclavian artery is mechanically compressed—often by a cervical rib, elongated C7 transverse process, or hypertrophied scalene/clavicular structures—creating focal arterial injury, post-stenotic dilatation, or true aneurysm formation. You will often present differently than a patient with neurogenic symptoms: instead of paresthesia, you may notice ischemic signs such as coolness, pallor, exercise-induced claudication of the hand, or even ulceration of fingertips if embolization has occurred. Because the blood flow to the tissues can quickly become dangerous, doctors use CTA or regular angiography early on to identify the problem; these imaging tests can show narrowing, aneurysms, blood clots in the artery wall, or blocks.
When you have arterial compression, the treatment strategy prioritizes restoring unobstructed arterial flow and preventing further embolization. Acute presentations with distal ischemia often need urgent endovascular or open thromboembolectomy to re-establish perfusion, followed by definitive decompression (resection of cervical rib or first rib and scalenectomy) and arterial reconstruction as indicated—this might include patch angioplasty, bypass, or resection of an aneurysmal segment. In groups of patients who receive both vascular repair and decompression, the chances of saving the limb are high if the treatment is done quickly, but waiting too long can lead to lasting damage to the fingers.
Surgical planning for you typically combines preoperative CTA, duplex evaluation, and sometimes catheter angiography to map thrombus and aneurysm. Postoperative care involves antiplatelet therapy or anticoagulation depending on the repair type, surveillance imaging to assess graft or arterial repair patency, and rehabilitation focusing on shoulder girdle mechanics to minimize recurrent compression. Outcomes hinge on a multidisciplinary approach—vascular surgery to address the arterial lesion, thoracic or orthopedic input for bony anomalies, and coordinated rehab to optimize shoulder posture and reduce recurrent stress on the repair.
For more information about arterial presentations, note that even subtle positional ischemia can precede frank embolic events, so attention to changes in pulse with provocative positioning and early vascular imaging often changes management from conservative to definitive surgical pathways.
Venous Thoracic Outlet Syndrome
Venous TOS usually happens when a blood clot forms in the axillosubclavian vein (known as Paget–Schroetter syndrome), and it often affects otherwise healthy young adults who do activities that involve lifting their arms a lot, like rowing, weightlifting, or manual labor Clinical hallmarks include sudden arm swelling, a heavy or aching sensation, cyanosis, and visible collateral veins across the shoulder or chest; in acute phases you may also have significant pain and limitation in use of the limb. Duplex ultrasound is the first-line diagnostic tool and can demonstrate venous occlusion, while catheter venography remains the gold standard for procedural planning and thrombolysis.
Treatment for venous TOS aims to clear thrombus, relieve mechanical compression, and prevent recurrence—this is often done in stages. If you present acutely, catheter-directed thrombolysis or pharmacomechanical thrombectomy within the first 7–14 days provides the best chance to restore vein patency and reduce post-thrombotic morbidity. Once the thrombus burden is reduced, definitive decompression—commonly first rib resection with scalenectomy and subclavian vein decompression—is performed to correct the underlying extrinsic cause; case series indicate improved long-term patency and functional outcomes when decompression follows timely thrombus clearance.
After intervention, your regimen usually includes short-term anticoagulation and close surveillance with duplex imaging; persistent venous stenosis may require patch angioplasty or venous reconstruction in select cases, but stenting across the thoracic outlet is generally avoided because ongoing extrinsic compression frequently leads to stent fracture or restenosis. Functional rehabilitation to correct scapular kinematics and reduce recurrent overhead compression plays an important role in reducing relapse, and you should be counseled on a staged return to sport or heavy labor with graded conditioning.
Additional points about venous cases: early decompression after thrombolysis—often within weeks—correlates with lower rates of post-thrombotic syndrome and recurrent thrombosis, and multidisciplinary coordination between vascular specialists, thoracic surgeons, and therapists improves both limb function and return-to-activity timelines.
Any new, severe, or progressive signs—acute limb swelling, loss of distal pulses, persistent cyanosis, or rapidly worsening neurologic deficit—require immediate evaluation at an emergency or vascular center.
Symptoms of Thoracic Outlet Syndrome
Neurological Symptoms
You will most often notice neurological signs because neurogenic TOS accounts for roughly 90–95% of symptomatic cases; those signs usually start as intermittent paresthesia and progress to persistent numbness and weakness. For example, you may feel tingling or “pins and needles” down the medial forearm into the ring and small fingers, and it can be worse with overhead reaching, carrying a heavy bag, or sleeping with your arm overhead. Electrophysiological testing (EMG/NCS) may later show denervation in the C8–T1 innervated intrinsic hand muscles, and in chronic untreated cases you might develop visible wasting of the hypothenar eminence or the interossei—what clinicians sometimes call a Gilliatt‑Sumner pattern of weakness.
You’ll also experience functional deficits before dramatic wasting appears: your grip strength can drop, you may frequently drop objects, and fine motor tasks like buttoning or typing become noticeably harder. Symptoms often fluctuate throughout the day; standing or sitting with forward head posture and rounded shoulders can precipitate a flare, while brief rest and position change may temporarily relieve symptoms. In athletes who do repetitive overhead activities—like swimmers, pitchers, and painters—nerve problems often show up sooner and are more serious because the constant use of the scalene or pectoralis minor muscles leads to tightness and pulls on the nerves
Clinical tests you undergo may include provocative maneuvers such as Roos (elevated arm stress test) or Adson’s test, which reproduce the paresthesia or diminish the radial pulse, suggesting compression of the brachial plexus elements. You should be aware that normal imaging or an unremarkable X‑ray does not exclude neurogenic involvement; diagnostic clarity often comes from combined clinical findings, EMG changes, and response to targeted interventions such as scalene muscle blocks or physical therapy focused on posture and scalene lengthening.
Vascular Symptoms
Vascular presentations divide into venous and arterial patterns, with distinct signs arising based on the affected area. If the blood flow from the veins is blocked (venous TOS, which happens in about 3–5% of cases), your arm might feel heavy and swollen after you use it a lot, and you may see bulging veins on your shoulder and chest; some people notice a bluish color and sudden swelling after doing something strenuous overhead, which doctors call effort thrombosis or Paget–Schröetter syndrome. In contrast, arterial compression (rare, around 1–2% of cases) produces coldness, pallor, decreased digital perfusion, and sometimes digital ulceration or finger ischemia when embolization occurs from a subclavian artery lesion.
You might be sent for duplex ultrasound, CT angiography, or venography when vascular symptoms are suspected; these studies can show axillosubclavian compression, thrombus, or arterial aneurysm. In venous TOS, acute thrombosis often requires urgent attention because you can develop extensive axillary‑subclavian clots that cause severe pain and functional immobility; a typical case report involves a young weightlifter who wakes with a blue, swollen dominant arm and is found to have a subclavian vein thrombus. With arterial TOS, you may notice exertional arm pain and then persistent fingertip numbness or coolness, and a physical exam can reveal a diminished or absent radial pulse with the arm in abduction or external rotation.
Management pathways differ because the vascular complications carry risks beyond localized symptoms: venous thrombosis can propagate or cause pulmonary embolism, and arterial thromboembolism can produce permanent digital ischemia. Your physician will treat the vascular emergency first (anticoagulation, thrombolysis when indicated) and then address the anatomic compressive source—so early recognition of vascular signs like dramatic swelling, cyanosis, absent pulses, or new ischemic pain is important for preventing long‑term damage.
You might have more than one sign of vascular issues at once; for instance, you could feel heaviness in your arm when you exert yourself due to venous congestion and also experience coolness in your arm from reduced blood flow if both blood vessels are being pressed on by a cervical rib or enlarged scalene muscle. Keeping track of pulses and blood flow patterns when you change positions helps identify which blood vessel is mainly affected, and quick imaging can show if you need immediate treatment before planning surgery to relieve pressure.
Pain and Discomfort
Pain patterns in TOS are varied and often multifocal: you may feel a deep, aching pain in the neck and trapezius, sharp or burning pain extending into the shoulder and down the arm, or occipital headaches originating at the base of the skull. Symptoms can mimic cervical radiculopathy or rotator cuff pathology, but the pain from TOS is frequently positional—worse with overhead activity, carrying items on one shoulder, or with prolonged computer work—and relieved partially by dropping the shoulder or changing head position. Pain intensity can range from a dull background ache to severe lancinating episodes that interrupt sleep.
You might also experience additional muscle pain from your muscles being tense for a long time: tight muscles in the front of your neck and chest can create painful spots that keep causing pain in the area and other places, while stiffness in the neck and upper back adds to ongoing discomfort that doesn’t go away with regular pain relievers. In some people, the pain evolves into neuropathic descriptors—burning, electric shocks, or allodynia—especially when the brachial plexus is chronically irritated. Clinicians often quantify your pain with numeric scales and functional questionnaires because the subjective intensity does not always correlate with objective findings, yet the impact on function is very real.
If stretching the scalene muscles and improving your posture greatly lessen your pain, it likely means the pain is caused by pressure related to your posture instead of a problem with your neck. If your pain continues even after trying various conservative treatments, doctors might need to use diagnostic injections (like a scalene block) or advanced imaging to determine if your pain is due to TOS or other issues and to decide if you should see a specialist for vascular or surgical evaluation.
More detailed pain characterization—timing, triggers, quality—helps your care team prioritize interventions. For instance, pain that wakes you at night and is associated with hand numbness points to neural compression, while discomfort that appears suddenly with arm swelling suggests a vascular event; documenting these temporal patterns accelerates correct treatment selection.
Impact on Daily Life
Your daily activities can be affected early and substantially, even with intermittent symptoms. Simple tasks like grooming, dressing, carrying groceries, or lifting a laptop become challenging when you experience arm weakness, numbness, or pain after short periods of use. Athletes and certain professionals—hairdressers, painters, manual laborers, and musicians—may see performance decline quickly because repetitive overhead activity both provokes symptoms and perpetuates the underlying muscle imbalance or compression. Often, you will adapt movements to avoid triggers, which can create compensatory strain elsewhere (shoulder impingement, thoracic dysfunction) and prolong recovery.
Sleep disturbance is common: you’ll often change positions frequently to find relief, and daytime fatigue follows, reducing work productivity and increasing irritability. Psychosocial impacts accumulate as well; chronic pain and functional loss are linked to anxiety, depression, and reduced engagement in hobbies. From a vocational standpoint, delayed diagnosis or inadequate workplace accommodations can force you to reduce hours, change jobs, or take medical leave—outcomes reported in case series of workers with longstanding TOS who required surgery after conservative measures failed.
Financial and healthcare burdens also rise with prolonged symptoms: repeated specialist visits, imaging, physical therapy courses, and possible anticoagulation or vascular interventions add up, and you may face weeks of reduced earning capacity after surgical decompression if that becomes necessary. Early ergonomic modification, structured physical therapy, and pacing strategies often prevent that trajectory, so documenting how symptoms limit your daily routines helps clinicians tailor a pragmatic rehabilitation plan that keeps you functional at work and home.
More specifically, small workplace changes—adjustable armrests, modified tool use, scheduled micro‑breaks, and task rotation—can restore many of your lost functions and prevent worsening; when these measures fail, objective functional decline over weeks to months often prompts escalation to imaging or procedural options.
Diagnosis of Thoracic Outlet Syndrome
Medical History and Physical Examination
You need a focused history that teases apart neurogenic, arterial and venous presentations, because management differs markedly. Ask about the onset (gradual versus sudden) and precipitating events such as a neck trauma, repetitive overhead work, or recent central venous catheterization; for example, effort-induced arm swelling and bluish discoloration after a rowing session suggest venous compression, whereas a cold, pale hand and exertional arm pain with diminished pulses point toward arterial involvement. Quantify symptoms: how often the paresthesia wakes you at night, whether a heavy lifting episode preceded onset, and any systemic signs such as unexplained arm swelling or claudication-like pain that limits exertion to minutes rather than hours.
You should perform a structured physical exam that combines inspection, palpation, and provocative maneuvers. Inspect for muscle atrophy in the thenar or intrinsic hand muscles, asymmetric venous distension, or a visible cervical rib bulge. Palpate the supraclavicular fossa and scalene triangle for tender trigger points and reproduce symptoms with targeted compression; in one case series, palpable scalene tenderness correlated with operative findings in a substantial subset of neurogenic patients. Then apply standardized provocative tests—Adson’s, Roos (EAST), Wright’s hyperabduction and the costoclavicular maneuver—while documenting pulse changes, symptom reproduction, and range-of-motion limits.
You must interpret provocative maneuvers cautiously because isolated positive tests are common in asymptomatic people and in cervical radiculopathy. Combine test results with the history: a positive Roos test plus objective findings such as neck pain radiating to the ulnar digits and intrinsic muscle weakness raises the pre-test probability of true neurogenic TOS and justifies further electrodiagnostic and imaging evaluation. Finally, use focused neurologic testing (sensory mapping, motor strength of C8–T1 innervated muscles like the first dorsal interosseous and abductor digiti minimi, and reflexes) to differentiate brachial plexus compression from peripheral entrapment or cervical root disease.
Imaging Techniques
You will order targeted imaging based on the suspected subtype: plain radiographs, ultrasound, CT angiography (CTA), MR angiography (MRA) and conventional catheter angiography each have distinct roles. Start with an upright chest and cervical spine x‑ray to look for osseous anomalies; a cervical rib is present in roughly 0.5–1% of the general population but is overrepresented in arterial TOS cohorts, so its identification changes your diagnostic pathway. For venous TOS, duplex ultrasound with dynamic arm positioning is a practical first-line study to demonstrate flow obstruction or thrombosis; a recent audit from a vascular clinic showed duplex identified subclavian vein compression or thrombosis in 85% of confirmed venous cases when performed with provocative maneuvers.
You should reserve CTA or MRA with arm provocation for suspected arterial or complex neurovascular compression because it provides high-resolution anatomical detail and detects aneurysms, intimal damage, or focal stenosis. CTA offers excellent spatial resolution and is faster, making it preferable when you suspect arterial thrombosis or need surgical planning, whereas MRA gives superior soft-tissue contrast for brachial plexus visualization without radiation exposure. In patients who have symptoms that come and go based on their position, using dynamic CTA/MRA with the arm raised can reveal blockages that aren’t seen when the arm is at rest; one study found that this type of imaging changed the surgical approach in about
You will also consider invasive catheter-based digital subtraction angiography (DSA) when noninvasive studies are inconclusive or when endovascular intervention is planned. DSA remains the gold standard for arterial anatomy and allows simultaneous therapeutic procedures such as thrombolysis or stenting in select arterial and venous presentations. Use venography with provocative maneuvers in suspected venous TOS to map thrombus extent and collateral circulation—this often guides whether first-line management is thrombolysis with subsequent decompression or anticoagulation alone.
More details on image interpretation matter: on x-rays, look not only for a complete cervical rib but also for hypoplastic ribs, anomalous first-rib morphology, or prominent transverse processes that reduce the scalene triangle volume. On duplex ultrasound, pay attention to peak systolic velocities and phasic flow changes with respiration and abduction—abrupt loss of phasicity or monophasic flow with arm elevation is highly suggestive of hemodynamically significant compression. When reviewing CTA/MRA, follow the entire subclavian artery and vein course through the thoracic outlet, document any post‑stenotic dilation, intraluminal thrombus or arterial wall irregularity, and compare supine versus upright or abducted arm positions if available.
Nerve Conduction Studies
You should order electrodiagnostic studies when neurogenic symptoms dominate or when the physical exam is equivocal between radiculopathy and lower brachial plexus compression. Standard testing includes sensory and motor nerve conduction studies (NCS) plus needle electromyography (EMG) targeted to C8–T1 innervated muscles such as the first dorsal interosseous, abductor digiti minimi and flexor carpi ulnaris. In true neurogenic TOS with lower trunk involvement, EMG often shows chronic denervation changes (fibrillations, reduced recruitment and large amplitude motor unit potentials) in these muscles, whereas routine median and ulnar motor conduction velocities may remain normal unless there is concomitant peripheral entrapment.
You need to incorporate specialized sensory studies because they can increase diagnostic yield: medial antebrachial cutaneous sensory nerve action potentials (SNAPs) are commonly assessed, and reduced amplitude on the symptomatic side supports lower trunk plexopathy. Sensitivity of electrodiagnostic testing varies; in surgical cohorts of confirmed neurogenic TOS, abnormal EMG/NCS findings are reported in roughly 30–70% of patients depending on the criteria used. Therefore, use electrodiagnostics to corroborate clinical suspicion and to document objective neurologic impairment prior to invasive interventions.
You must also use EMG/NCS to exclude mimics such as C8–T1 radiculopathy, ulnar neuropathy at the elbow, and peripheral neuropathies; compare paraspinal muscle EMG to limb muscle findings to distinguish plexus from root disease. Repeated tests can provide useful information: seeing better muscle activity and fewer abnormal signals after treatment or injections can show that the patient is improving. When planning surgery, looking at the initial electrodiagnostic problems can help predict how well a patient will recover afterward; more severe chronic denervation seen on preoperative EMG is linked to slower or incomplete
More info on technical execution: perform studies both at rest and after provocative maneuvers when possible—for example, compare SNAP amplitudes with the arm neutral versus abducted, because dynamic compression can produce position-dependent changes that standard supine testing misses. Ensure temperature control and normative data for age and limb length, and document side-to-side amplitude differences greater than 20–30% as potentially significant. Finally, coordinate electrodiagnostic timing with imaging and clinical findings so that all data inform a cohesive diagnosis and treatment plan.
Treatments for Thoracic Outlet Syndrome
Conservative Treatments
You should start with targeted physical therapy focused on posture correction, scapular stabilization and progressive strengthening of the rotator cuff and periscapular muscles; typical protocols call for 2–3 supervised sessions per week and a home program, with meaningful improvement often seen in 6–12 weeks. In practice you’ll work on stretching the anterior chest (pectoralis minor) and scalene muscles, retraining cervical and thoracic posture, and performing neural gliding exercises to reduce traction on the brachial plexus. Clinical studies generally show that about 50–75% of patients with neurogenic TOS feel better after following a structured rehab program, but how well it works can depend on how long they’ve had symptoms and any physical pressure on their nerves.
You can augment manual therapy with soft-tissue techniques aimed at trigger points in the scalene, levator scapulae and pectoralis muscles; dry needling and myofascial release can decrease local myofascial pain and improve range of motion when performed by a trained clinician. Acupuncture is another adjunct that some studies and clinic series show reduces pain scores and improves function over 4–8 sessions; its effect size is modest but useful when combined with exercise and ergonomics. Ergonomic changes at work—raising monitors, adjusting chair height, and avoiding overhead work for prolonged periods—often produce measurable relief within weeks when paired with active rehabilitation.
You should consider diagnostic and therapeutic injections before escalating care: Ultrasound-guided injections into the scalene or pectoralis minor muscles with a local anesthetic can help determine if surgery will be beneficial by temporarily easing pain Botulinum toxin injections into the anterior scalene or pectoralis minor can help relax the muscles and relieve symptoms for 3 to 6 months in some patients, but the effects don’t last long, and you may need more injections; avoid using botulinum toxin if you have neuromuscular disorders (like myasthenia gravis), an active infection where you’re injecting, or if you’re taking certain blood thinners without proper precautions Homeopathic remedies have not shown reliable objective benefit in trials and should be viewed only as supportive adjuncts rather than primary therapy.
Medical Interventions
You will commonly be prescribed medications to manage pain and neuropathic symptoms: nonsteroidal anti-inflammatory drugs (NSAIDs) for inflammatory pain, short courses of muscle relaxants for spasms, and neuropathic agents such as gabapentin or pregabalin when paresthesia or burning pain predominates (the typical starting gabapentin dose is 300 mg at night, titrated as needed). For cases involving deep vein thrombosis (like effort thrombosis or Paget–Schroetter syndrome), the usual treatment is anticoagulation, starting with low-molecular-weight heparin and then switching to an oral anticoagulant for about 3 months, while arterial thoracic outlet syndrome (TOS) with Outcomes vary by type: pharmacologic therapy relieves symptoms reliably in inflammatory or mild compressive cases, while vascular TOS requires a combined medical and procedural approach.
You can use image-guided injections both diagnostically and therapeutically: corticosteroid injections around inflamed soft tissues may reduce localized swelling and pain for weeks to months, and diagnostic scalene blocks with lidocaine are strongly predictive of improved outcomes following decompression surgery when they produce clear short-term relief. Botulinum toxin injections are sometimes employed as both a therapeutic trial and symptom relief measure; studies and clinic series show variable duration and magnitude of benefit, so you should use them as part of a stepwise plan rather than a long-term sole strategy. Vascular interventions include catheter-directed thrombolysis for acute venous thrombosis followed by definitive decompression, and percutaneous angioplasty or stenting is generally avoided as a first-line solution for dynamic compression because restenosis or device failure rates are high when the mechanical cause isn’t corrected.
Additional options such as spinal cord stimulation are available for refractory neuropathic pain after other measures have failed; you’ll usually undergo a temporary trial (days to weeks) before permanent implantation, and small case series report meaningful pain reduction for selected patients with persistent neuropathic symptoms post-decompression. Use of neuromodulation requires a multidisciplinary assessment—pain specialist, neurosurgeon, or physiatrist—and you should weigh expected pain relief against device risks like infection or lead migration. Overall, match the medical intervention to the TOS subtype: neurogenic TOS responds best to neuromodulatory and neuropathic pain strategies, venous TOS to anticoagulation and thrombolysis, and arterial TOS to vascular repair combined with decompression.
Surgical Options
You should consider surgery when you’ve failed an adequate trial of conservative care (commonly 3–6 months) and you continue to have functional limitation, progressive neurologic deficit, or vascular compromise; vascular presentations—acute venous thrombosis or arterial embolization—often prompt more urgent operative management. The most common operations are: first rib resection with scalenectomy, pectoralis minor release, and decompression of fibrous bands. Results for vascular TOS after surgery to relieve pressure and fix blood vessels are very good in many studies, showing that 80–95% of patients feel better or function better, while improvement in neurogenic TOS varies but is often significant, with 60–80% of carefully chosen cases showing progress.
You’ll encounter several surgical approaches, each with advantages and trade-offs: The transaxillary approach offers direct access to the first rib through a cosmetically hidden incision, but it limits exposure for complex vascular reconstruction. On the other hand, the supraclavicular approach allows for better control of blood vessels and options for repairs (like patching or bypassing arteries) while giving easier access to cervical ribs and the brach For extensive disease, combined approaches may be necessary. In venous TOS with chronic subclavian vein scarring, you may need thrombectomy, venoplasty, or patch venoplasty in addition to decompression; in arterial TOS, you frequently require arterial reconstruction or bypass following decompression if there is intimal damage or aneurysm formation. Expect perioperative complications in a minority of cases—pneumothorax, transient brachial plexus symptoms, wound issues—and discuss these risks with your surgical team.
Postoperative rehabilitation shapes your long-term outcome: early gentle range-of-motion within 1–2 weeks, progressive strengthening from 4–6 weeks, and full functional recovery over 3–12 months are typical. You’ll typically see marked improvement in strength and reduction in paresthesia within months if decompression successfully relieves mechanical pressure; persistent neuropathic pain occurs in a subset and may require adjunctive pain management or neuromodulation. Reoperation rates are low, but they can happen if there is still some bone or tissue pressing on nerves, and it’s important to have long-term check-ups with vascular imaging or electrodiagnostics if vascular reconstruction was done during the surgery
Before surgery, it’s important to gather information: get specific imaging tests (like duplex ultrasound or CT/MR angiography for blood vessel issues) and nerve tests if neurogenic TOS is suspected, and use a diagnostic scalene block to help predict if surgery will You’ll do best when surgery is part of a multidisciplinary plan—with a vascular surgeon, a thoracic surgeon, or a neurosurgeon, as indicated—so that the specific anatomy, subtype (neurogenic, venous, or arterial), and your functional goals determine the exact procedure and timing.
Holistic Treatments for Thoracic Outlet Syndrome
Acupuncture
You can use acupuncture to help with both pain and nerve issues in thoracic outlet syndrome by stimulating specific points in the neck and shoulder areas that affect the upper body and nervous system. In practice, doctors typically select certain points on the neck and shoulders, such as GB21, SI12, and points on the Small Intestine and Large Intestine channels, along with other points that help with pain and blood flow, like LI4 and LV3. Typical protocols in clinical reports involve 1–2 sessions per week for 6–8 weeks; many patients report measurable pain reduction after the first 3–4 sessions, with some case series noting 30–50% decreases in pain scores and improvements in paresthesia and hand dexterity when acupuncture is added to multimodal care.
You can expect the practitioner to use a combination of local needling and techniques like auricular or electroacupuncture for stubborn symptoms: using low-frequency electrostimulation (2–4 Hz) can improve blood flow to the nerves and has been linked to less tightness in the scalene and pectoralis minor muscles. If you have neurogenic TOS, the treatment often includes specific ear points and methods to help calm the nervous system, while for vascular TOS, the focus is on techniques that improve blood flow. Adverse events are uncommon, but you should inform your acupuncturist about any use of anticoagulants or implantable devices to avoid complications.
You will see the best results when acupuncture is combined with other treatments like specific physical therapy and improving your posture; while there isn’t a lot of strong research, some studies show that acupuncture can help reduce pain medication use and improve how well you function. If your symptoms include significant arterial compromise (coolness, pallor, diminished pulses) or acute venous thrombosis signs, acupuncture should be deferred or performed only after vascular clearance. Track objective measures—pain intensity on a 0–10 scale, grip strength, and frequency of paresthesia—so you can assess progress across 6–12 weeks.
Chiropractic Care
You might find chiropractic care helpful, which focuses on gentle movements of the neck and upper back, relaxing tight muscles, and retraining your nerves to ease tension in specific areas like the scalene, levator scapulae, In many treatment plans, chiropractors combine gentle spinal adjustments with tools that help relax soft tissues to improve how joints move and ensure the shoulder blades work properly; these programs usually involve 6 to 12 visits over 4 to 8 weeks, and many patients notice better movement and less pain by visits 4 to 6. A case series of manual therapy for neurogenic TOS reports symptom relief in a substantial portion of patients when interventions are combined with home exercises and ergonomic adjustments.
You should make sure the chiropractor screens for vascular involvement and neurological red flags before high-velocity thrusts, because arterial or venous TOS and signs of plexus compression change the risk–benefit profile of some manipulative techniques. When vascular compromise is suspected—cortical limb coolness, diminished distal pulses, or acute swelling—the practitioner should refer you for duplex ultrasound or vascular consultation. For most people with neurogenic or mild positional TOS, gentle movements, exercises to stabilize the shoulder blades, and techniques to help the nerves can help reduce pain and improve symptoms without needing strong manipulation.
You will see better long-term outcomes when chiropractic care is part of a staged program: initial pain control and mobility restoration followed by progressive strengthening and motor-control retraining. Clinics use objective measures like the Disabilities of the Arm, Shoulder and Hand (DASH) score, pain ratings, and range-of-motion assessments; many reports show these measures improve within 6–12 weeks when chiropractic care is combined with exercise and posture correction.
More info: When you evaluate chiropractors, ask about experience managing thoracic outlet presentations specifically, whether they use instrument-assisted soft tissue mobilization (IASTM), and if they employ outcome tracking. Request a conservative trial focused on gentle mobilization and neuromuscular re-education rather than immediate high-velocity manipulations, and ensure communication lines are open with your physical therapist or vascular specialist if symptoms evolve.
Homeopathic Remedies
You can think about using homeopathic remedies as a safe, extra option to help with symptom flare-ups and muscle soreness from thoracic outlet syndrome; common treatments include Arnica montana for soreness after manipulation, Ruta graveolens for tendon irritation, and Hypericum perforatum for nerve pain. In practice, practitioners choose remedies based on the symptoms; for instance, if a patient has sharp pains in the arm, they might suggest Hypericum 30C, while if someone feels deep muscle soreness after using their muscles too much, they might recommend Arnica 200C or 30C. Dosage schedules vary widely, but typical regimens involve a single dose repeated every 24–48 hours initially, then as needed based on symptom response.
You should be aware that high-quality trials specifically for homeopathy in thoracic outlet syndrome are lacking, and evidence is mostly anecdotal or from small observational reports; nevertheless, many patients report subjective reductions in muscle tightness, improved sleep, and less reliance on over-the-counter analgesics when a homeopathic plan is combined with physical therapy and lifestyle changes. Practitioners sometimes integrate constitutional prescribing—matching a remedy to your overall physical and psychological profile—alongside acute remedies aimed at discrete symptom patterns, which can be helpful if you have fluctuating symptoms that vary with stress or hormonal cycles.
You will want to communicate any homeopathic use with your other providers to avoid confusion in tracking outcomes and to ensure it complements rather than replaces interventions with stronger evidence bases, such as exercise therapy and manual techniques. If you are pregnant, breastfeeding, or taking other medications, discuss homeopathic selections with a qualified practitioner; although direct pharmacologic interactions are rare with homeopathic potencies, coordinated care improves safety and effectiveness.
More info: Typical homeopathic practice for musculoskeletal complaints emphasizes individualized treatment and short follow-up intervals; if you pursue homeopathy, track symptom diaries (pain intensity, paresthesia frequency, functional limitations) over 4–8 weeks to determine whether the remedy produces clinically meaningful change alongside other therapies.
Lifestyle Changes
You will get measurable benefit by changing daily habits that perpetuate neurovascular compression: optimize your workstation so your shoulders are relaxed with elbows at roughly 90 degrees, raise monitors to eye level to avoid forward head posture, and swap heavy shoulder bags for backpacks or cross-body carriers that distribute weight away from the thoracic outlet. Simple adjustments—for example, limiting overhead reaching to under 10–15 minutes per activity session and taking microbreaks every 30–45 minutes—reduce cumulative load on the scalene and pectoralis minor muscles. In observational cohorts, patients who adopt ergonomic changes alongside home exercise programs report faster symptom improvement, often within 4–8 weeks, versus those who continue high-risk postures.
You should commit to targeted daily exercises that address length and strength imbalances: scalene and pec minor stretches held for 30 seconds and repeated 3 times, twice daily; scapular retractions (10–15 reps, 2–3 sets) performed every other day; and progressive rotator cuff strengthening using 1–3 kg resistance bands to rebuild endurance. Neural gliding exercises tailored to your symptoms—for example, gentle median or ulnar nerve glides—help desensitize irritated brachial plexus fibers when done 3–4 times daily for 10 repetitions. Weight management and aerobic conditioning also matter: reducing excess adiposity around the neck and thorax and improving microvascular function through 20–30 minutes of moderate aerobic exercise 3–5 times per week can reduce inflammatory contributors to pain and paresthesia.
You will need to monitor activity modifications and sleep posture: avoid sleeping with your arm overhead and use a cervical roll to maintain a neutral neck alignment. Small behavior changes compound over time, so set concrete goals—for example, perform the stretching routine every morning for 8 weeks and log adherence; many patients report decreased nighttime numbness and fewer positional flares within that timeframe. If your job requires repetitive overhead tasks or heavy lifting, discuss temporary duty modifications with your employer and seek an occupational health assessment to implement sustainable ergonomic controls.
More info: Ergonomic interventions can be quantified—adjust chair height so your hips are slightly above knees, keep the keyboard 10–15 cm from the torso, and set the monitor top at eye level—and combine these with a progressive home exercise plan that you reassess every 4 weeks to ensure steady functional gains.
Benefits of a Holistic Approach
You will see a significant decrease in symptoms by tackling several causes of thoracic outlet syndrome at the same time: manual therapies relieve muscle pressure, exercise improves movement control, acupuncture helps manage pain, and lifestyle changes eliminate ongoing physical stress. In integrated care pathways, many patients find they need less pain medication and get better faster than with just one type of treatment; clinics that use multiple approaches often see clients making noticeable improvements in pain and function within 6–12 weeks when treatments are organized together. This multimodal structure also helps you pinpoint which component delivers the greatest benefit by using objective outcome measures, such as pain scores, DASH, grip strength, and sleep quality indices.
You should expect improved long-term outcomes because holistic care focuses on the drivers of recurrence: persistent postural strain, uncorrected scapular dyskinesis, and unresolved trigger points. By combining symptom-focused treatments with preventive measures, you lower the likelihood of chronic central sensitization and reduce the need to escalate to invasive procedures. For example, programs that pair manual therapy and exercise with daily ergonomics and stress management report higher patient satisfaction and lower rates of surgical referral compared with conventional care alone.
You will also experience secondary benefits beyond symptom relief—better sleep, reduced anxiety around activity, and improved tolerance for work and recreational tasks—which translate into measurable quality-of-life gains. Tracking progress with validated scales and periodic reassessment allows you and your care team to adapt the plan, intensify rehabilitation if needed, or pursue specialized vascular or surgical evaluation for arterial or venous presentations that do not respond to conservative measures.
More info: To maximize the advantages of a holistic plan, implement measurable goals (pain ≤3/10, DASH improvement of ≥10 points, or return to specific activity) and reassess every 4–8 weeks so you can escalate, taper, or maintain interventions based on objective progress.
Final Words
With this in mind, you should understand that thoracic outlet syndrome (TOS) is not a single disease but a pattern of symptoms produced when neurovascular structures are compressed as they exit the thorax. Your symptoms and how bad they are depend on the type of TOS: neurogenic TOS causes pain, numbness, tingling, and weakness in the arm and hand; venous TOS can lead to swelling, blue skin, and blood clots; arterial TOS might make your arm feel cold, look pale, have weak pulses, and suffer Common anatomic and functional causes include cervical ribs or fibrous bands, scalene or pectoralis minor muscle hypertrophy or spasm, trauma, repetitive overhead activity, and sustained poor posture. Diagnosis typically relies on a combination of careful clinical examination and targeted testing—plain radiographs, CT or MR angiography, Doppler ultrasound for vascular assessment, and electrodiagnostic studies when neurogenic compression is suspected—because the management you receive needs to be tailored to the underlying mechanism and severity of compression.
You should pursue a staged treatment strategy that prioritizes conservative measures, because many people experience meaningful improvement without surgery. Physical therapy that focuses on posture correction, scapular stabilization, scalene and pectoralis minor stretching, progressive strengthening and myofascial trigger point release is the foundation of care. Nerve blocks in the scalene or pectoralis minor muscles can help identify the source of pain and provide temporary relief; botulinum toxin injections into the scalene muscles may also be used for diagnosis or treatment, but they have risks like certain medical conditions, infections at the injection site, allergies, and pregnancy, and should only be given by skilled doctors. Acupuncture may serve as an adjunct for symptom control for some patients, while homeopathic remedies lack robust evidence and should not replace evidence-based interventions. Spinal cord stimulation is sometimes looked at for severe nerve pain that doesn’t get better with other treatments, but there isn’t much evidence for its use in people with thoracic outlet For cases with ongoing nerve problems or serious blood flow issues, surgeons who are skilled in TOS may perform surgery to relieve pressure, usually by removing the first rib or releasing certain muscles, but this comes with specific risks that you need to talk about in detail.
You should engage in shared decision-making with a multidisciplinary team so that management matches your goals, symptom patterns, and risk tolerance. Keep an eye out for red flags, such as rapidly worsening weakness, signs of acute limb ischemia, and marked swelling suggestive of venous thrombosis, which necessitate immediate evaluation. TOS does not cause systemic conditions like hypertension or hormonal changes like menopause, and there is no evidence that TOS triggers early menopause. Expect rehabilitation to take weeks to months, adhere to progressive activity modification and ergonomic strategies, and consider adjunctive modalities (manual therapy, acupuncture) when they are provided by qualified practitioners. When conservative care proves inadequate, discuss the indications, expected benefits and potential complications of interventional or surgical options so you can pursue a clear, evidence-based path toward functional recovery.
FAQ

Q: What is thoracic outlet syndrome (TOS) and which structures are affected?
A: Thoracic outlet syndrome is a group of disorders caused by compression of neurovascular structures as they exit the thorax through the thoracic outlet. Structures commonly involved are the brachial plexus (neurogenic TOS), the subclavian vein (venous TOS), and the subclavian artery (arterial TOS). Compression can arise from anatomical variants (cervical rib, anomalous scalene muscles), trauma, repetitive overhead activity, poor posture, or hypertrophy/scar tissue around muscles and ligaments.
Q: What are the three main types of TOS and how do they differ?
A: The three types are neurogenic, venous, and arterial. Neurogenic TOS (most common) involves brachial plexus irritation producing pain, numbness, weakness, and paresthesia. Venous TOS involves subclavian/axillary vein compression causing arm swelling, cyanosis, pain, and sometimes effort thrombosis (Paget–Schroetter syndrome). Arterial TOS involves subclavian artery compression producing ischemic symptoms: coldness, pallor, diminished pulses, claudication, and risk of distal embolization.
Q: What are common symptoms that suggest each TOS type?
A: Neurogenic: arm/hand numbness, tingling, burning, weakness, muscle wasting in severe cases, and pain radiating from neck/shoulder. Venous: sudden arm swelling, heaviness, blue discoloration, prominent veins, pain, and stiffness after exertion. Arterial: cold or pale hand, diminished or absent pulse, claudication with use, pain at rest in advanced cases, and possible fingertip ulceration or embolic events.
Q: Can thoracic outlet syndrome cause high blood pressure or early menopause?
A: TOS does not typically cause systemic hypertension; compression is localized to the subclavian vessels and nerves and rarely produces sustained systemic blood-pressure elevation. TOS does not induce early menopause or ovarian failure; there exists no physiological mechanism connecting thoracic outlet compression to premature menstrual cessation or ovarian hormone depletion.
Q: What are some natural and conservative ways to treat TOS?
A: First-line management emphasizes noninvasive approaches: tailored physical therapy (posture correction, scapular stabilization, neural gliding, scalene and pectoralis stretching), activity modification and ergonomic changes, myofascial release and trigger-point therapy, breathing retraining, therapeutic massage, heat/ice and anti-inflammatory measures, and acupuncture for pain relief. Lifestyle measures include weight management and gradual return to activity. Evidence quality varies; multidisciplinary care guided by a clinician is recommended.
Q: What are the main uses of injections, nerve blocks, Botox, and spinal cord stimulation? What are some important reasons not to use them?
A: Diagnostic or therapeutic nerve blocks (scalene or brachial plexus region) can localize pain sources and provide temporary relief; contraindications include infection at the site, uncontrolled bleeding disorder, or allergy to agents. Botulinum toxin injections into the scalene or pectoralis muscles can help reduce muscle spasms in certain nerve-related cases; however, they should not be used if you have neuromuscular disorders (like myasthenia). Spinal cord stimulation is rarely used for refractory neuropathic pain after other measures fail; benefit is case-dependent and evidence is limited. All interventions carry risks and should be considered with specialist input.
Q: When is surgery necessary for TOS, and what types of surgery are done?
A: Surgery is an option when conservative care doesn’t work, when there is a progressive neurological deficit or significant vascular compromise, or when there is recurrent venous thrombosis or arterial ischemia. Common procedures include first-rib resection, scalenectomy (anterior and middle scalene removal), cervicothoracic decompression for anatomical anomalies, and vascular reconstruction (thrombectomy, patch angioplasty, bypass) when arteries or veins are damaged. Risks include nerve injury, pneumothorax, bleeding, infection, persistent symptoms, and the need for further procedures.
Holistic treatment for TOS in Philadelphia
Homeopathy and acupuncture are two of the most effective treatments for thoracic outlet syndrome, especially when combined together. At the Philadelphia Holistic Clinic, Dr. Tsan uses traditional homeopathy, acupuncture, and homeosiatry.
Contact Philadelphia Homeopathic Clinic at (267) 403-3085 to book an appointment for a homeopathic evaluation with Dr. Tsan.