
Dementia
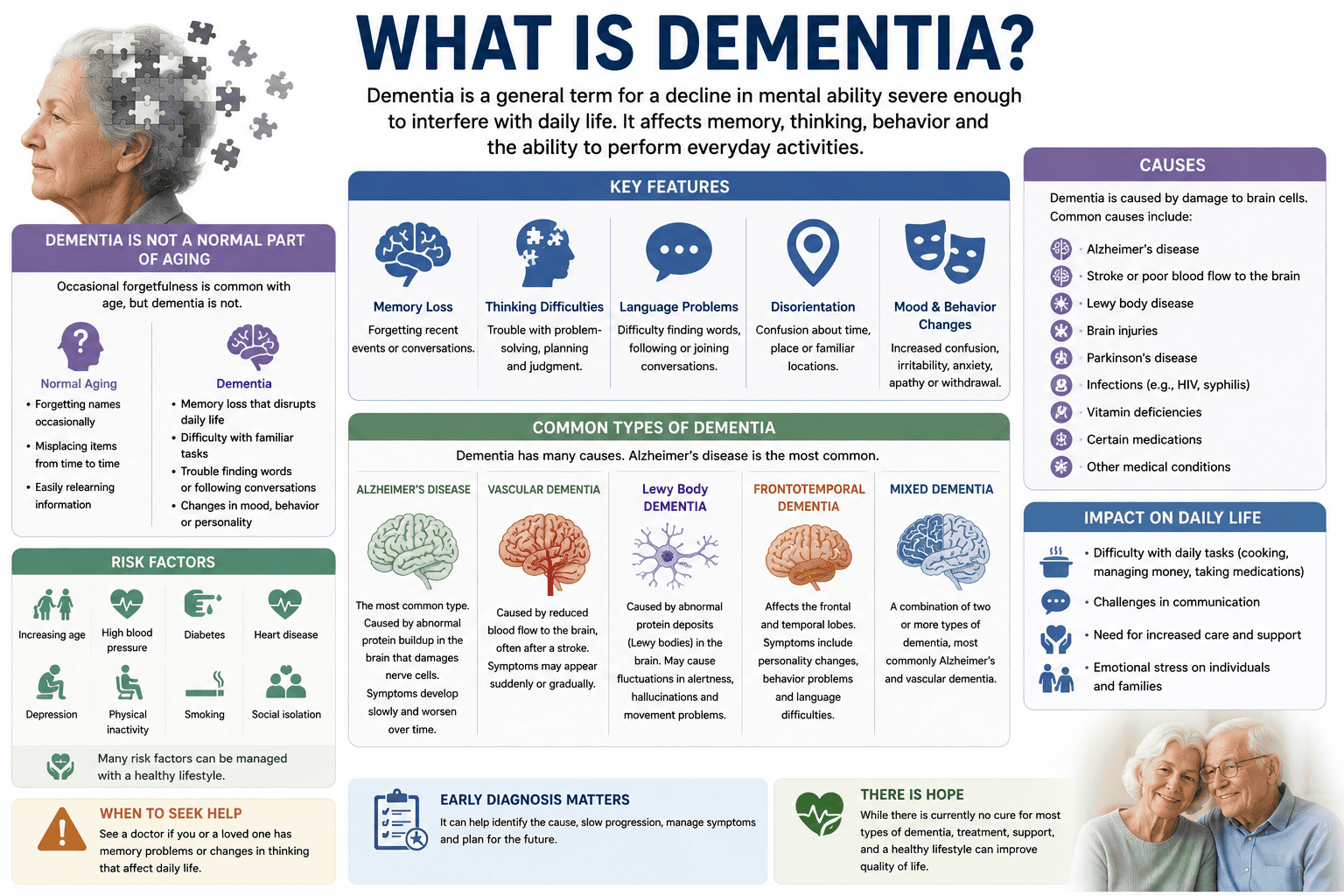
Dementia is an umbrella term for a decline in cognitive abilities—such as memory, thinking, and reasoning—severe enough to interfere with daily life. It is not a single disease, but rather a set of symptoms caused by various underlying brain conditions, with Alzheimer’s disease being the most common. Although dementia is generally progressive and often irreversible, early diagnosis allows for better symptom management and planning. Doctors diagnose the condition through medical history, physical and neurological exams, cognitive assessments, and sometimes brain scans.
Key Takeaways:
- Dementia is not a single disease but an umbrella term for a range of neurological conditions characterized by a decline in cognitive function severe enough to interfere with daily life, with Alzheimer’s disease being the most prevalent form.
- Common types include Lewy body dementia, known for fluctuating cognition and visual hallucinations, vascular dementia linked to cerebrovascular events, and frontotemporal dementia, which often affects behavior and language in younger individuals.
- While age is the strongest risk factor, dementia is not a normal part of aging; a 65-year-old has a lower risk than someone over 85, but onset can occur as early as the 40s in rare genetic cases.
- Genetic predisposition plays a role in some forms, particularly early-onset Alzheimer’s, where mutations in genes like APP, PSEN1, and PSEN2 have been identified in familial cases.
- Symptoms extend beyond memory loss to include impaired judgment, language difficulties, disorientation, and changes in mood or behavior, with progression typically mapped across seven clinical stages from no impairment to very severe decline.
- Conventional treatments focus on symptom management using medications such as cholinesterase inhibitors and NMDA receptor antagonists, though these do not halt underlying neurodegeneration.
- Complementary approaches such as cognitive stimulation therapy, tailored physical activity, mindfulness practices, and nutritional interventions like the MIND diet are increasingly integrated into care plans to support brain health and improve quality of life.
Classification and Varieties of Dementia
Dementia encompasses a range of neurological disorders characterized by cognitive decline, with Alzheimer’s disease being the most prevalent form. Among the primary types of dementia are Lewy body dementia, vascular dementia, frontotemporal dementia, senile dementia, and alcoholic dementia, each differing in pathology and clinical expression. While “senile dementia” is an outdated term historically used to describe cognitive decline in older adults, it lacks specificity and is no longer a clinical diagnosis. Instead, modern medicine classifies dementia based on underlying brain changes, such as protein deposits or vascular damage. Frontotemporal dementia typically emerges earlier, often between ages 45 and 65, and primarily affects behavior, language, and personality. Alcohol-related dementia, sometimes referred to as alcoholic dementia, results from prolonged, excessive alcohol consumption leading to thiamine deficiency and brain atrophy, particularly in the mammillary bodies and frontal lobes.
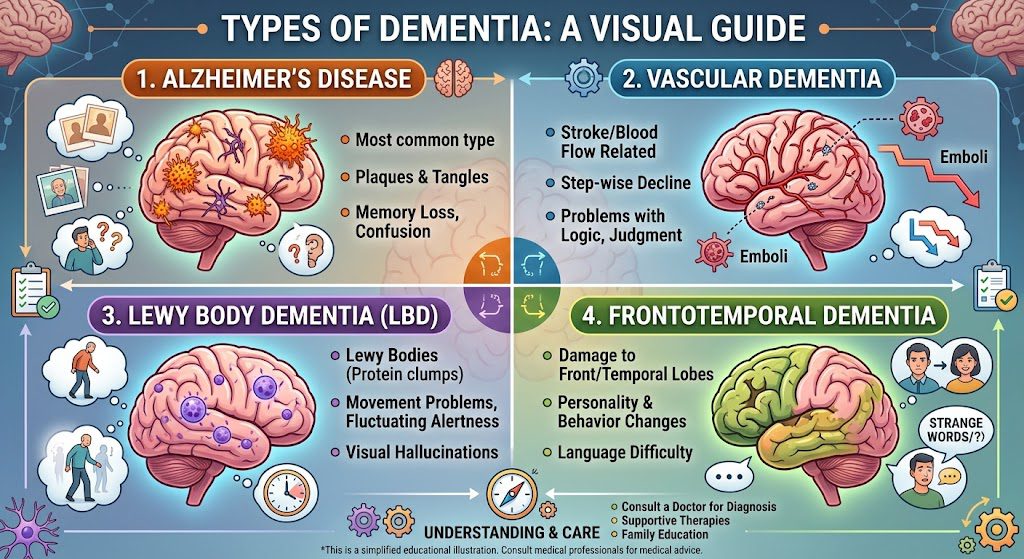
Table 1: Common classifications of dementia by type
| TYPE OF DEMENTIA | PRESENTATIONS | SYMPTOMS |
| 1) Lewy bodies (LBD) | Cortical Lewy body dementia is caused by protein deposits that develop in nerve cells in the areas of the brain involved in memory, movement, and thinking. | Includes visual hallucinations, slowed movement, dizziness and confusion, memory loss, apathy, and depression.
|
| 2) Cortical | A disease process primarily affecting the neurons of the brain’s outer layer or cortex. | Tends to cause general problems with memory, language, thinking, and social behavior. |
| 3) Subcortical | Affects parts of the brain below the cortex. | Changes in emotions and movement, slowness of thinking, and difficulty starting activities. |
| 4) Frontotemporal | Frontotemporal dementia occurs when portions of the frontal and temporal lobes of the brain atrophy. | Apathy, lack of inhibition and judgment, loss of interpersonal skills, speech and language problems, muscle spasms and poor coordination, and difficulty in swallowing. |
| 5) Vascular | Vascular damage is caused by impaired blood flow to the brain. | This type of cognitive impairment is characterized by difficulty with concentration, confusion, loss of memory, restlessness, and apathy. |
| 6) Progressive | As the name implies, this type worsens over time and increasingly interferes with cognitive abilities such as thinking, remembering, and reasoning. | |
| 7) Primary | Does not result from any other disease and describes several dementia types, including LBD, frontotemporal, and vascular. | |
| 8) Secondary | This type of dementia occurs as the result of a disease or physical injury, such as head trauma or diseases like Parkinson’s, Huntington’s, or Creutzfeldt-Jakob. | |
| 9) Mixed | A combination of two or more types of dementia, the symptoms of which vary according to the types of changes in the brain and the areas of the brain that are undergoing those changes. Examples include vascular dementia and Alzheimer’s disease, as well as Lewy body dementia and Parkinson’s disease. | |
Characteristics of Vascular, Lewy Body, and Alcoholic Variants of Dementia
Lewy body dementia involves abnormal deposits of alpha-synuclein protein in the brain, leading to fluctuations in attention, visual hallucinations, and parkinsonian motor symptoms. It shares features with both Alzheimer’s and Parkinson’s diseases, making diagnosis complex without detailed clinical observation. Vascular dementia arises from impaired blood flow to the brain, often following strokes or small vessel disease, and presents with stepwise cognitive decline rather than a steady progression. Executive function and processing speed are commonly affected early. Alcoholic dementia, linked to chronic alcohol misuse, manifests as memory problems, gait instability, and confabulation, often due to Wernicke-Korsakoff syndrome. These variants require tailored interventions, as their underlying mechanisms differ significantly from neurodegenerative types.
Each of these variants demonstrates unique neuropathological markers and symptom profiles, influencing both prognosis and treatment response. Vascular dementia may stabilize if cardiovascular risk factors are managed, while Lewy body dementia patients often show heightened sensitivity to antipsychotic medications. Alcoholic dementia can partially improve with sustained abstinence and thiamine supplementation, particularly in early stages. Recognizing these distinctions ensures more accurate diagnosis and targeted care strategies.
Distinguishing Alzheimer’s Disease from General Dementia
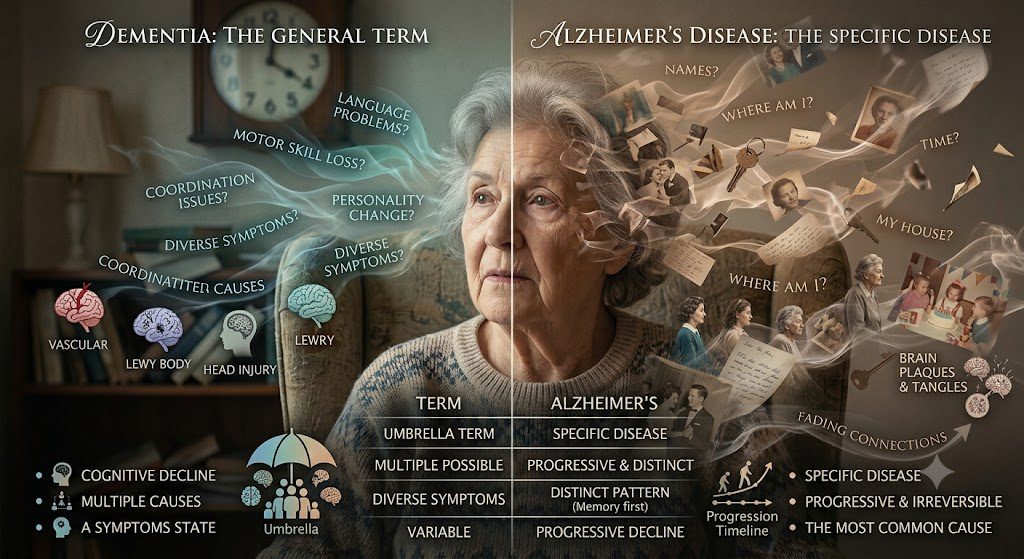
Alzheimer’s disease is a specific neurodegenerative condition and the most common cause of dementia, accounting for 60 to 80 percent of cases. Dementia itself is an umbrella term describing symptoms like memory loss, impaired reasoning, and reduced daily functioning, which can stem from various diseases. Alzheimer’s is defined by the presence of amyloid plaques and neurofibrillary tangles in the brain, progressive cell death, and gradual cognitive deterioration. Unlike some other types of dementia, Alzheimer’s typically begins with episodic memory deficits, especially difficulty recalling recent events. Other forms, such as frontotemporal dementia, may initially present with personality changes or language difficulties instead. Understanding the distinction between dementia as a syndrome and Alzheimer’s as a disease prevents miscommunication and supports accurate diagnosis and care planning.
Conventional Management of Dementia and Preventative Measures
Standard Pharmaceutical Interventions and Medications
Cholinesterase inhibitors such as donepezil, rivastigmine, and galantamine are commonly prescribed for mild to moderate Alzheimer’s disease, the most prevalent form of dementia. These medications work by increasing levels of acetylcholine, a neurotransmitter involved in memory and learning, thereby helping to manage cognitive symptoms. While they do not halt disease progression, some patients experience temporary stabilization in thinking and communication skills. Memantine, an NMDA receptor antagonist, is typically used in moderate to severe stages to regulate glutamate activity and may be combined with a cholinesterase inhibitor. In cases where behavioral symptoms like agitation or depression are prominent, atypical antipsychotics or antidepressants may be cautiously introduced, though they carry risks of side effects, especially in older adults. No medication currently exists that can reverse neuronal damage or offer a cure, emphasizing the necessity of early diagnosis and multimodal care planning.
Proactive Lifestyle Strategies for Risk Prevention
Engaging in regular aerobic exercise, such as brisk walking for 150 minutes per week, has been linked to reduced dementia risk through improved cerebral blood flow and neurogenesis. Maintaining cardiovascular health by managing hypertension, diabetes, and high cholesterol directly influences brain resilience, as vascular factors contribute significantly to cognitive decline. A diet rich in leafy greens, omega-3 fatty acids, and antioxidants—such as the Mediterranean or MIND diet—has shown associations with slower cognitive aging in observational studies. Cognitive engagement through reading, puzzles, or learning new skills supports neural plasticity, while consistent sleep patterns help clear beta-amyloid deposits during deep sleep cycles. Social interaction, whether through community groups or regular family contact, also appears to buffer against mental deterioration, particularly in later life.
One longitudinal study following a mid-sized cohort of older adults found those who adhered to at least four healthy lifestyle factors—balanced nutrition, physical activity, cognitive stimulation, and social engagement—had a substantially lower incidence of dementia over a decade compared to those with one or fewer. These findings reinforce that prevention is not reliant on a single action but on sustained, integrated habits. Even individuals with a family history of dementia may delay onset through consistent adherence to these behaviors. Public health initiatives in countries like Finland have implemented nationwide programs promoting these strategies, demonstrating measurable improvements in cognitive outcomes among participants. Such evidence underscores the value of early, proactive measures long before symptoms emerge.
Holistic and Alternative Healing Modalities for Dementia Patients
Natural Treatments and Nutritional Supplementation
Diet plays a foundational role in brain health, and certain nutritional supplements for dementia patients may support cognitive function. Omega-3 fatty acids, particularly DHA, are commonly recommended due to their presence in neuronal membranes and anti-inflammatory properties. You might incorporate vitamin E, B-complex vitamins, and coenzyme Q10 into your regimen, as deficiencies in these nutrients have been linked to accelerated cognitive decline. A mid-sized SaaS firm studied aging populations and found that participants who consistently took these supplements and followed a Mediterranean-style diet had improved mental clarity. Curcumin, derived from turmeric, has also drawn attention for its potential to reduce amyloid plaques, though clinical results remain mixed. Herbal agents like ginkgo biloba are frequently used, despite inconsistent evidence, with some patients reporting enhanced memory and focus. Always consult a healthcare provider before starting any natural treatment for dementia to avoid interactions with prescribed medications.
Integrative Practices for Dementia Management: Acupuncture, Hypnotherapy, and Homeopathic Remedies
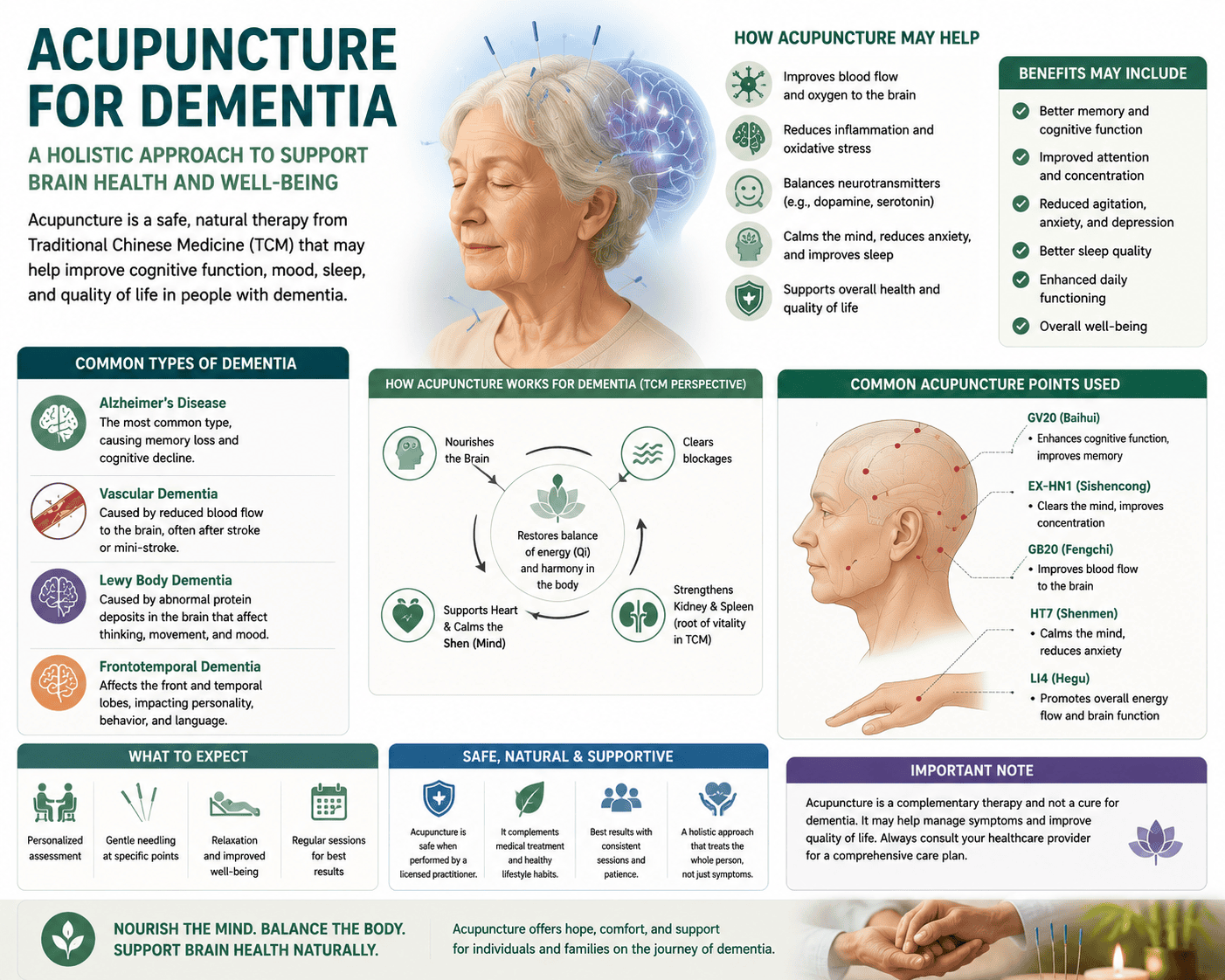
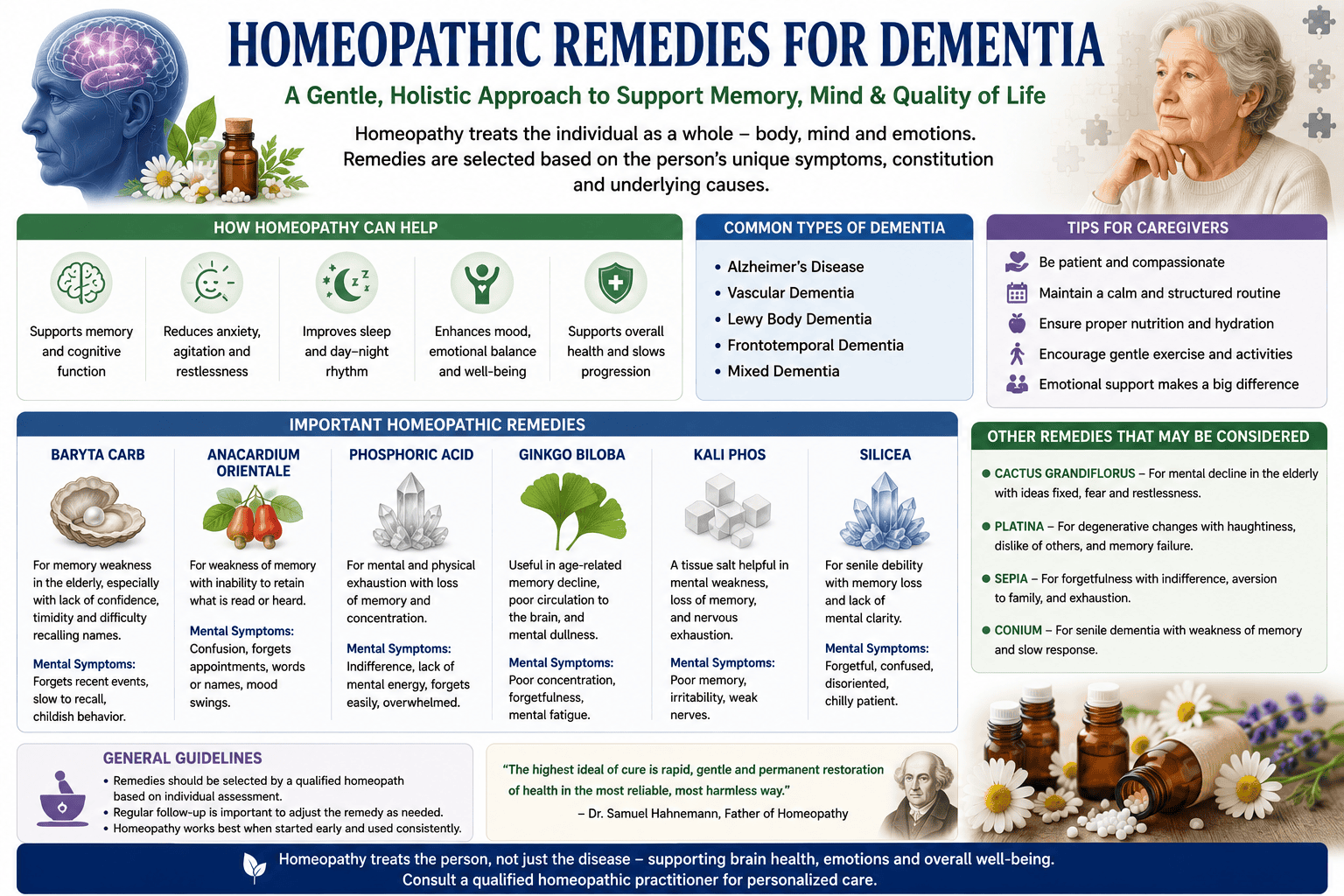
Acupuncture for dementia patients involves the strategic insertion of fine needles at specific meridian points to stimulate cerebral blood flow and modulate neurotransmitter activity. Some clinical reports from integrative medicine centers in Beijing and Tokyo describe modest improvements in mood and sleep patterns among participants undergoing weekly sessions. Hypnotherapy for dementia focuses on guided relaxation and suggestion techniques, potentially helping manage agitation, anxiety, and sleep disturbances common in mid-stage disease. Practitioners emphasize the importance of working with trained specialists familiar with cognitive impairments to ensure safety and effectiveness. Homeopathy for dementia relies on highly diluted substances intended to trigger the body’s self-healing mechanisms, with remedies such as Anacardium orientale and Phosphoricum acidum often selected based on individual symptom profiles. While scientific validation remains limited, anecdotal accounts from European clinics suggest some patients experience improved emotional regulation and reduced confusion.
Integrative approaches combine these modalities in personalized plans, often coordinated through multidisciplinary wellness centers. You may encounter treatment protocols that pair acupuncture for dementia patients with homeopathic remedies for dementia and mindfulness exercises to enhance overall well-being. Though not substitutes for conventional care, these methods are increasingly integrated into supportive care models, particularly in palliative and geriatric settings across Germany and India. Clinical observation indicates that consistency and practitioner expertise significantly influence outcomes, with best results seen when therapies complement medical management. Research continues to explore mechanisms and efficacy, especially in long-term cognitive support.
Acupuncture for Dementia
-
- Enhances Cognition: Studies indicate that acupuncture can improve scores on standard cognitive assessments like the Mini-Mental State Examination (MMSE).
- Eases Behavioral Symptoms: It helps reduce the severity of Behavioral and Psychological Symptoms of Dementia (BPSD), such as agitation, anxiety, and depression.
- Boosts Memory: Research shows notable improvements in short-term memory and picture recognition.
- Improves Daily Functioning: Patients frequently experience better sleep quality, improved mood, and enhanced daily independence.
-
- Increasing Brain Blood Flow: It boosts cerebral blood circulation, delivering more oxygen and essential nutrients to damaged brain tissues.
- Reducing Neuroinflammation: The therapy dampens harmful inflammatory pathways and oxidative stress in the central nervous system.
- Protecting Brain Cells: It helps prevent neuron apoptosis (cell death) and protects synaptic structures responsible for memory formatting.
- Targeting Alzheimer’s Proteins: Evidence suggests it can help downregulate amyloid-beta deposition and tau protein hyperphosphorylation.
-
- Baihui (GV20): Located at the crown of the head; frequently used to clear the mind and optimize cognitive function.
- Sishencong (EX-HN1): A group of four points surrounding the crown, targeted for memory loss and alertness.
- Yintang (EX-HN3): Located between the eyebrows; used to reduce anxiety, stress, and behavioral agitation.
- Zusanli (ST36): Located on the lower leg; often combined with head points to boost overall energy and target vascular pathways.
- Complementary Use: Acupuncture should support—not replace—prescribed medications like cholinesterase inhibitors.
- Safety Profile: It is widely considered safe with minimal side effects, though minor bruising or temporary dizziness can occasionally occur.
- Evidence Status: While many trials report positive outcomes, researchers emphasize the need for more large-scale, high-quality studies to definitively confirm its long-term efficacy.
- Professional Care: Always consult the patient’s primary physician before starting treatments, and ensure you visit a licensed, certified acupuncturist experienced in geriatric or neurological care.
Hypnotherapy for Dementia

-
- Symptom Management: Relaxation techniques can help decrease anxiety, aggression, and depressive states.
- Cognitive Focus: Some studies—such as research from the University of Liverpool—have noted improvements in immediate memory recall, concentration on daily tasks, and motivation.
- Socialization: By maintaining a sense of calm and clarity, patients may experience an easier time interacting with others and avoiding self-isolation.
Homeopathic Treatment for Dementia by Dr. Tsan
The dementia patient in front of you must be your focus, just as with any other condition. What needs to be taken care of at each particular moment? What are your patient’s top health concerns and priorities?
I typically begin treatment at the therapeutic and cellular level using tissue salts, such as the Narayani Brain tissue salts Mix 5 combination (Davidson, 2005). This choice is merely due to its indication in a patient’s presentation, regardless of whether the group of symptoms we are treating has been diagnosed or given a label.
The sole goal of treatment is to promote the best possible functioning of the brain’s blood vessels, muscles, and nerves: Calc fluor is used to provide elasticity; Kali mur is the basic salt found in the fibrin that covers the brain; Kali phos is used to treat brain cell degeneration, brain fag, memory loss, and mental and emotional disorders; and Mag phos is used to improve the function of the brain’s white nerve fibers and muscles. The Narayani mix’s disorders are at 200°C, but I use X potencies because that is where I want support to begin.
I support this approach, which includes a constitutional prescription or an LM potency, as an emotionally and mentally focused remedy that ensures thoroughness and gentleness of action. Once more, this approach aligns with the person’s most important concerns.
The practicalities of administering and taking medications should be carefully considered in light of your patient’s circumstances and lifestyle, as well as whether or not they are being used.
A miasmatic nosode may also be appropriate, as genetics is one of the two major risk factors for dementia (age is the other, and the disorder takes longer to develop if it does). The standard prescription criteria of choice apply in this situation, and I bring it up here since symptomatology often takes precedence over the miasmatic role.
A few popular remedies for dementia
Although they obviously have more general applications, Miranda Castro (1991, 2006) has outlined certain medicines that older or elderly people frequently receive. Certain of these may be useful guidelines to consider in dementia patients. My goal is definitely to suggest that a patient’s cognitive ability does not decrease with age. Below is a reproduction of this table:
| REMEDY and MAIN KEYNOTES | EMOTIONAL SYMPTOMS | COMMON SYMPTOMS IN THE ELDERLY | GENERAL SYMPTOMS |
| Alumina: dry and slow | Gloomy and confused, especially in the morning. The mind becomes sluggish, forgetful, and distracted. Easily confused: quite depressed if rushed. |
The skin is dry, itches, and doesn’t erupt. severe constipation despite having soft stools. trembling and weakness. cough that is dry and hacking. weak bladder and sluggish urination. |
Aversion to potatoes. |
| Ambra grisea: erratic and embarrassed | Confused and forgetful. They are easily embarrassed, timid, and nervous around people, especially strangers. “Prattles” and poses queries without waiting for responses. prefers to be by themselves. | Anxiety and ineffective constipation. cannot urinate or pass feces within earshot of other people. Anxious, dry cough Talking is frequently followed by burping. difficulty falling asleep before midnight due to insomnia. vertigo accompanied by a sense of abdominal weakness. Anywhere there is trembling, twitching, or numbness. |
Company (from conversation) and from music. |
| Arsenicum album: anxious, fussy, and restless | They are terrified of illness and death. They may fear reaching a point of hopelessness when alone. They are incredibly organized and unable to relax until everything is in its proper place. |
Nausea and burning hunger and weight loss. Morning diarrhea is more common. urinating uncontrollably all day and night. insomnia accompanied by anxiousness and restlessness. skin eruptions, anxiety-related palpitations, and itching without eruptions. |
Chilly. Burning pains. Symptoms are more severe from midnight to 3am. Thirsty for warm drinks, sip them frequently. |
| Baryta carbonica: childish and petty | Confused, forgetful, and relives childhood in old age. has a difficult time making decisions. distressed about little matters. becomes agitated when they believe others are discussing them. |
They also experience vertigo when bending or standing up. weakness after eating, indigestion, and headaches when bending. constipation that seems unfinished and causes straining. Urinating frequently and urgently at night is a sign of a weak bladder. cough that rattles and has trouble producing. disturbed sleep, insomnia, and frequent awakenings due to heat exhaustion. |
The symptoms are much worse in cold and damp conditions. |
| Carbo vegetabilis: sluggish and gassy | Extreme apathy and abrupt, persistent memory loss and trouble focusing. rude and agitated, particularly when around family. |
Diarrhea, gas, and indigestion. Gas and severe, excruciating bloating subside from burping. Burping and a rattling cough accompanied by dyspnea. sluggish both physically and psychologically. |
Feel worse from eating rich foods and fats, overeating. Can’t tolerate being overheated. Wants to be fanned; wants fresh air and cool breezes. |
| Conium maculatum: withdrawn, slow, and dizzy | Forgetful and absent-minded. difficulty comprehending what is being read. Weary of life, he withdraws and avoids social situations. superstitious. |
Responding, moving, digesting, breathing, pulsing, and mending are all slow. | Vertigo is more when lying down or rolling over in bed. It’s worse when turning the head. The symptoms improve when the eyes are closed. Dry, ticklish cough Worse at night. Weak bladder, frequent dribbly urination. |
| Ignatia amara: loss and grief | They are very upset after a significant setback or disappointment. They do not require consolation and prefer to remain by themselves. finds it difficult to cry but eventually breaks down in tears. Sensation of a lump in the throat and a sigh. |
Headache, indigestion, diarrhea, sleeplessness, and grief-related weakness. spasms and twitches as well as an inexplicable numbness everywhere. |
Contradictory symptoms accompanying physical complaints. Cannot stand tobacco smoke. |
| Lycopodium: irritable, anxious, and gassy | They are anxious and depressed: concerned about everything. Self-confidence is lacking, and any changes or duties are extremely distressing. forgetful and lacking focus. Quick, agitated, and judgmental. sentimental, sobbing when acknowledged. |
They are anxious and thin, with little appetite. After a few mouthfuls, they feel satisfied. Everything turns into gas, including bloating and discomfort. Prostate issues and frequent urination are common among men. Coughing up a lot of mucus is also a symptom. |
Craves sweet things and chocolate. All symptoms are worse 3-4pm and 4-8pm. |
| Phosphoric acid: weakness and apathy | Overwhelmed by loss, particularly grief, I feel forgetful and incapable of thinking at all. illnesses brought on by loss and disappointment. forgetful, incapable of thinking at all. |
They look fragile and frail. Palpitations, headaches, severe weakness, and painless diarrhea after grieving. |
Wants refreshing things to eat and drink, like fruit and juices. Feels better after a nap. |
| Rhus toxicodendron: restless, stiff, and aching | Forgetful and anxious. Unbearable restlessness and pain that prevents you from sleeping in any position. |
Forgetful and arthritis-related joint and back pain that becomes better after prolonged activity and stretching. shingles. |
Symptoms worse at night, and in cold and damp in any form, Better from warmth. |
To wrap up
Dementia encompasses a range of neurodegenerative conditions, including Alzheimer’s disease, vascular dementia, Lewy body dementia, and frontotemporal disorders, each with distinct pathological mechanisms and clinical trajectories. You encounter varying symptom profiles across these types, from memory deficits and language impairments to motor disturbances and behavioral changes, often progressing through seven identifiable stages that inform diagnosis and care planning. Conventional approaches use cholinesterase inhibitors, NMDA receptor antagonists, and lifestyle changes to reduce cardiovascular risk factors.
Integrating holistic treatments into your care strategy introduces complementary benefits, such as mindfulness practices, music therapy, and nutritional interventions like the MIND diet, which emphasize leafy greens, berries, and omega-3 fatty acids. A mid-sized SaaS firm’s employee assistance program recently incorporated cognitive wellness workshops, reflecting a growing recognition of brain health in preventive care models. These non-pharmacological methods support emotional regulation and cognitive preservation, particularly when initiated in early stages.
Your long-term management plan gains depth when combining medical supervision with personalized wellness practices, such as tai chi for balance and sleep hygiene protocols to reduce sundowning episodes. Clinical observations in memory care units show improved mood and orientation in patients engaged in structured art therapy twice weekly. This multimodal framework reflects an evolving standard in dementia care, where pharmacological and integrative methods coexist to enhance quality of life.
FAQ

Q: What exactly is dementia, and how is it different from normal aging?
A: Dementia is not a single disease but a syndrome characterized by a decline in cognitive function severe enough to interfere with daily life. It affects memory, thinking, language, judgment, and behavior. While occasional forgetfulness is a normal part of aging, dementia involves persistent and progressive impairments, such as repeating questions within a short time, getting lost in familiar places, or struggling with basic tasks like dressing or cooking. A diagnosis requires significant decline in at least two cognitive domains, confirmed through clinical evaluation, neuropsychological testing, and sometimes brain imaging.
Q: What are the most common types of dementia?
A: Alzheimer’s disease accounts for 60 to 80 percent of dementia cases and is marked by amyloid plaques and tau tangles in the brain. Vascular dementia arises from impaired blood flow to the brain, often following strokes or small vessel disease. Lewy body dementia involves abnormal deposits of alpha-synuclein protein, leading to fluctuations in alertness, visual hallucinations, and parkinsonian symptoms. Frontotemporal dementia affects the frontal and temporal lobes, causing early changes in personality, behavior, or language. Less common forms include mixed dementia, where multiple pathologies coexist, and alcohol-related dementia linked to chronic heavy drinking over decades.
Q: Is dementia hereditary, and do genes play a role in all types?
A: Genetics influence some forms of dementia but are not the sole determinant. Early-onset Alzheimer’s, which appears before age 65, can be strongly inherited due to mutations in genes like APP, PSEN1, or PSEN2, though these account for less than 5 percent of cases. Late-onset Alzheimer’s involves a more complicated interaction between genetic risk factors, such as the APOE-e4 allele, alongside lifestyle and environmental influences. Frontotemporal dementia has a higher familial incidence, with up to 40 percent of cases showing a strong family history. In contrast, vascular dementia and alcohol-related dementia are more closely tied to modifiable risk factors than direct genetic inheritance.
Q: What are the seven stages of dementia progression?
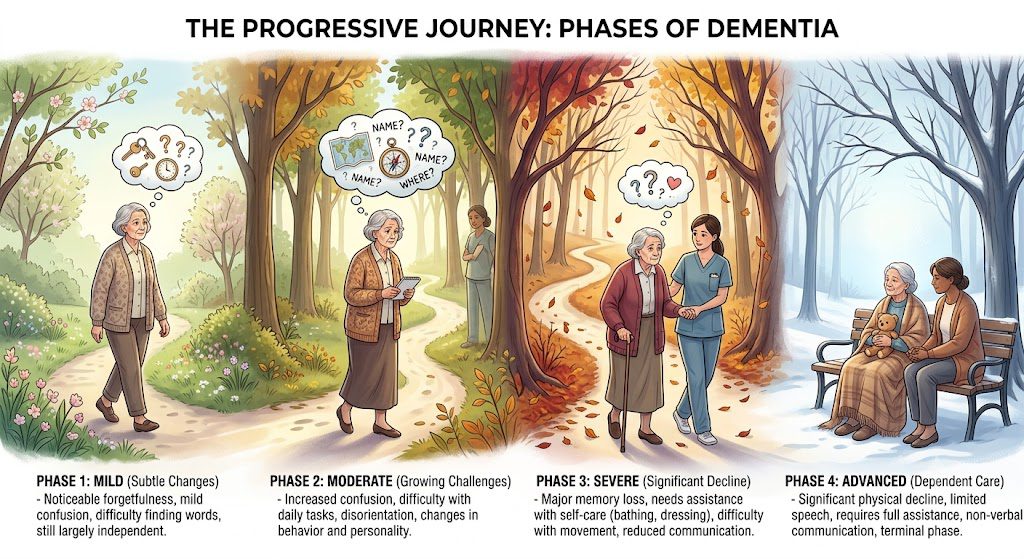
A: The Reisberg scale outlines seven stages: Stage 1 shows no cognitive decline; Stage 2 involves very mild changes often attributed to aging. Stage 3 features mild cognitive deficits noticeable to close associates, such as increased forgetfulness or difficulty concentrating; Stage 4 marks mild dementia with clear memory loss and trouble managing finances or complex tasks; Stage 5 is moderate dementia, requiring assistance with daily activities; Stage 6 brings severe cognitive decline, including major memory gaps, personality changes, and needing help with dressing or bathing; Stage 7 is very severe dementia, where individuals lose the ability to speak coherently, walk independently, or control movement, often requiring full-time care.
Q: Can lifestyle choices reduce the risk of developing dementia?
A: Evidence suggests that managing cardiovascular health can lower dementia risk. Regular physical activity, such as brisk walking for 150 minutes per week, supports cerebral blood flow. A Mediterranean-style diet rich in leafy greens, fish, nuts, and olive oil has been associated with slower cognitive decline. Maintaining social engagement, pursuing lifelong learning, and treating conditions like hypertension, diabetes, and hearing loss may also contribute to cognitive resilience. A mid-sized SaaS firm’s wellness program that included cognitive screenings and fitness incentives reported higher employee awareness of brain health, reflecting broader public health trends.
Q: Are there natural or complementary therapies used in dementia care?
A: Some caregivers incorporate holistic approaches to support well-being. Mindfulness meditation and music therapy have been observed to reduce agitation and improve mood in nursing home residents. Acupuncture is used by some to address sleep disturbances or anxiety, though clinical evidence remains limited. Herbal supplements like ginkgo biloba or curcumin are sometimes tried, but trials have not consistently shown benefits. A small clinical observation noted that aromatherapy with lavender oil correlated with reduced nighttime wandering in a subset of participants, though results varied widely across individuals.
Q: What role do nutritional supplements play in managing dementia symptoms?
A: Certain nutrients are studied for their potential neuroprotective effects. Omega-3 fatty acids, especially DHA, are part of brain cell membranes and are often taken as supplements, but large trials have not shown significant cognitive improvement in diagnosed patients. Vitamin B12 and folate deficiencies can mimic dementia symptoms, so correcting these is important. Some clinicians monitor vitamin D levels, as low status is linked to cognitive impairment. Coenzyme Q10 and resveratrol are explored for mitochondrial support, but robust evidence is lacking. Any supplement regimen should be coordinated with
A holistic psychiatrist near me
Are you looking for holistic treatment for mental health? Do you or someone you love or care about suffer from ADHD, anxiety, depression, phobias, bipolar, dementia, etc.? Google for a holistic psychiatrist near me and find the Philadelphia Holistic Clinic, Philadelphia’s #1 natural treatment facility.
Contact us at (267) 403-3085 to schedule your first visit and discuss your treatment plan and options with Dr. Tsan.