Prostatitis
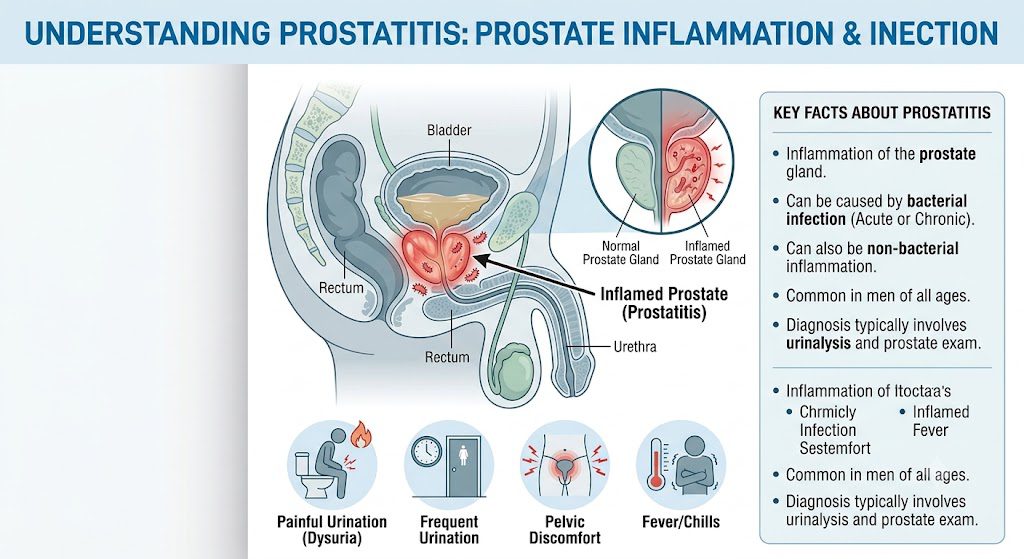
Just know that prostatitis refers to inflammation of the prostate, which is often labeled a prostate infection. Prostatitis is the inflammation or infection of the prostate gland. It frequently causes painful urination, frequent urges to urinate, and pelvic or lower back pain. Treatment depends on the underlying cause and may involve antibiotics, pain relievers, or lifestyle changes. You should monitor pelvic pain, urinary changes, or fever and consult a urologist for diagnosis and tailored treatment options.
Key Takeaways:
- Bacterial infection most commonly causes acute prostatitis, usually due to an ascending urinary pathogen or following instrumentation, such as catheterization, as seen in post-catheterization cases in hospital practice.
- Nonbacterial chronic pelvic pain syndrome involves inflammatory and neurogenic components and often presents without a positive urine culture, with pelvic floor tenderness on digital rectal exam a typical finding.
- Sexual transmission of prostate infection is uncommon, with sexually transmitted organisms more likely to cause urethritis in younger men than classic prostatitis, such as presentations after unprotected intercourse.
- In acute bacterial cases, the clinical presentation includes high fever, rigors, and severe dysuria. In chronic cases, it includes intermittent pelvic pain, ejaculatory discomfort, urinary frequency, and nocturia. Nocturia and perineal ache often lead to evaluation.
- Diagnosis depends on a focused rectal exam, urine analysis and culture, and targeted specimen collection such as pre- and post-prostatic massage samples when chronic bacterial prostatitis is suspected, with validated symptom scores used to quantify severity.
- Conventional management of acute bacterial prostatitis requires prompt antibiotics and sometimes inpatient care with parenteral therapy, whereas chronic bacterial prostatitis typically involves prolonged oral antibiotics, often prescribed for several weeks to months and frequently including fluoroquinolones or trimethoprim-sulfamethoxazole.
- Holistic and complementary options that may reduce symptoms include pelvic floor physiotherapy with biofeedback and myofascial release, alpha-blockers for voiding symptoms, timed bladder training, and selected phytotherapeutics, while acupuncture and homeopathic trials have convincing clinical support; pelvic physiotherapy is commonly delivered over multiple sessions by specialized therapists.
Etiology of Prostatitis and Transmission Pathways
How do you get a prostate infection? You most commonly acquire one when bacteria ascend from the urethra or bladder into the prostatic ducts, often after urinary retention, recent catheterization, or urologic procedures. Clinical histories from outpatient clinics frequently note onset within days of instrumentation, making procedural exposure a practical red flag.
Can a prostate infection be sexually transmitted? You can develop prostatitis from sexually transmitted pathogens such as Neisseria gonorrhoeae or Chlamydia trachomatis, particularly in younger, sexually active men, though many cases still stem from enteric organisms. Assessment of sexual history and recent urethritis helps distinguish an STI-related case from an enteric-source infection.
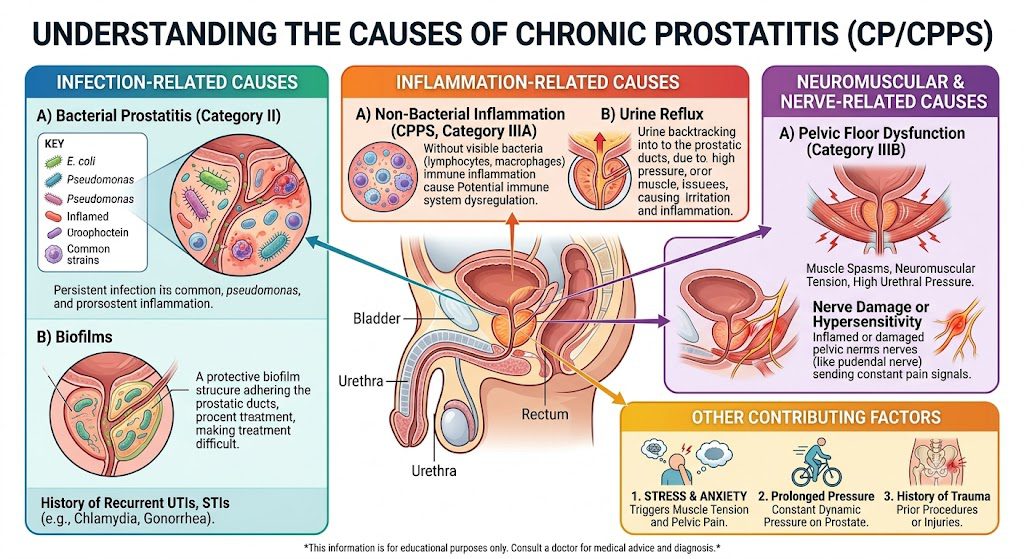
What is the most common cause of prostatitis? You are most likely dealing with bacterial prostatitis driven by gram-negative enteric organisms, with Escherichia coli reported most often in urine and prostatic secretion cultures. Chronic nonbacterial pelvic pain syndromes account for many chronic presentations, while acute symptomatic cases more reliably yield bacterial isolates such as E. coli.
Primary Bacterial Drivers
Escherichia coli is the organism most frequently isolated in acute bacterial prostatitis, and you will often identify matching strains in concurrent urinary tract infections. Clinical practice commonly links fever and perineal pain with positive E. coli cultures in urine, guiding initial empirical therapy selections in outpatient and inpatient settings.
Other enteric pathogens, including Proteus, Klebsiella, and Enterococcus species, also cause prostatitis, and you should expand culture interpretation when first-line therapy fails or when the patient has healthcare exposure. Pseudomonas and Staphylococcus aureus appear less often but are relevant after instrumentation or in nosocomial contexts.
Chronic bacterial prostatitis frequently shows recurrent isolates and biofilm formation, so you may observe months of relapsing symptoms with the same organism on expressed prostatic secretion cultures. Management complexity often reflects reduced antimicrobial penetration and bacterial persistence within prostatic tissue.
Modes of Contraction and Risk Factors
Ascending infection from the urethra or bladder represents the primary mode of contraction, so you should suspect prostate involvement following a complicated lower urinary tract infection. Procedures such as catheterization and cystoscopy provide direct access for microorganisms to colonize the gland.
Obstruction from benign prostatic hyperplasia or urethral stricture causes urine to stay in the bladder and bacteria to build up, which raises your risk of prostatitis if reflux into the prostatic ducts happens. Additional situational risks include recent prostate biopsy, pelvic trauma, and systemic conditions that impair host defenses.
Behaviors and exposures like unprotected sex, recent untreated urethritis, or frequent catheter use elevate the probability you will acquire an infection from sexually transmitted organisms or enteric bacteria, particularly in younger adults. Comorbidities such as diabetes further modify clinical risk and recovery patterns.
Consider the following contributors you should assess during history-taking and risk stratification:
- Recent urinary instrumentation or indwelling catheter use
- History of recurrent urinary tract infections
- Benign prostatic hyperplasia or other causes of urinary obstruction
- Recent sexually transmitted infection or untreated urethritis
- Immunosuppression or metabolic disease such as diabetes
- Recent prostate biopsy or pelvic trauma
This information helps you prioritize diagnostic testing such as urine culture, expressed prostatic secretion analysis, or nucleic acid amplification tests for STIs before initiating empirical therapy, for example, ordering a urine culture prior to antibiotics.
Signs and Symptoms of Chronic Prostatitis
-
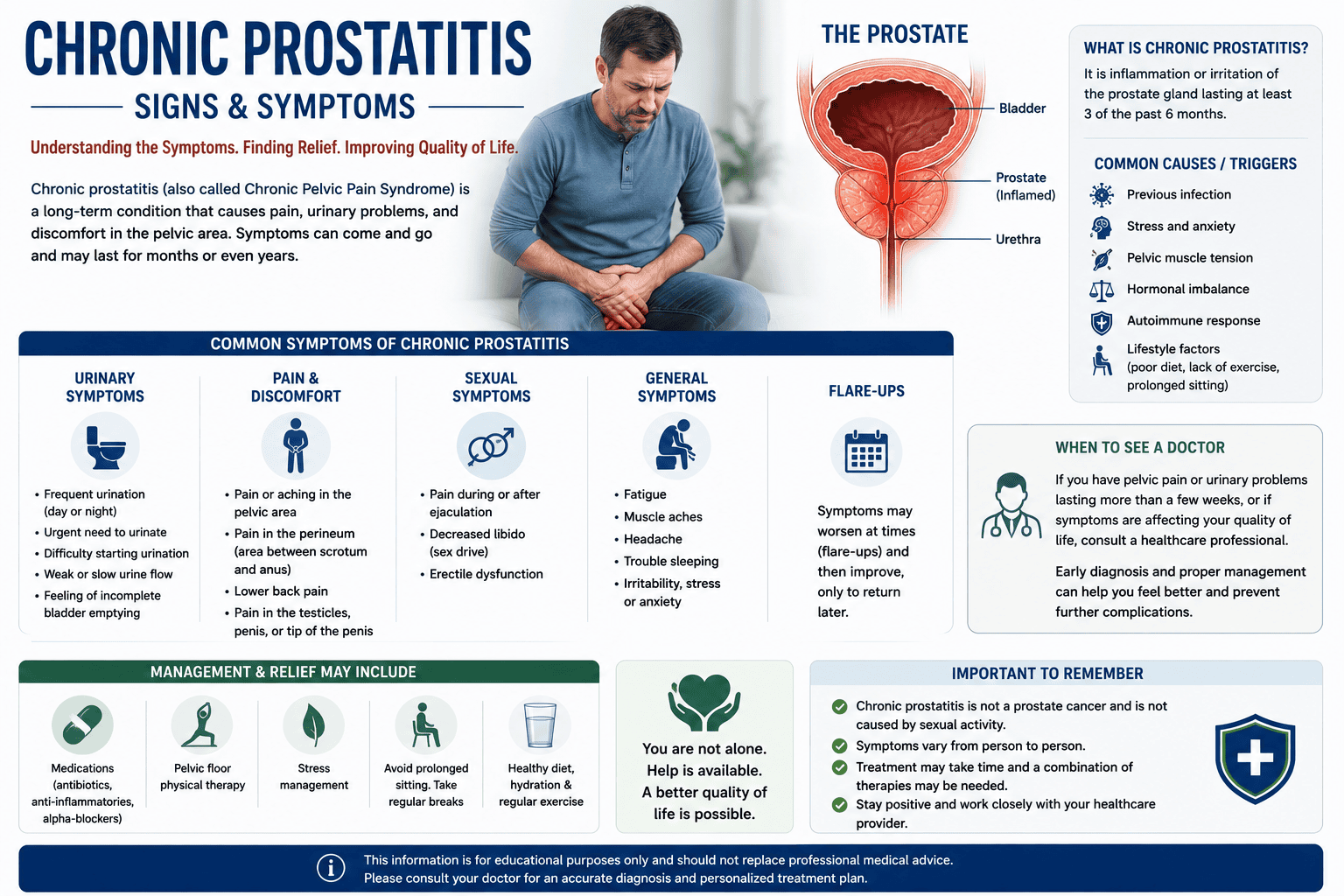
- Urinary Changes: Burning or pain when urinating, difficulty starting a urine stream, weak flow, and an urgent or frequent need to go, including getting up frequently at night.
- Pain: A dull ache in the lower abdomen, groin, lower back, or perineum (the area between the scrotum and rectum).
- Sexual Discomfort: Pain during or immediately following ejaculation.
- Systemic Signs: Recurring urinary tract infections (UTIs) and sometimes low-grade fever, chills, and body aches.
- Persistent Pain: Throbbing or aching pain in the pelvis, genitals, anus, and low back.
- Irritative Voiding: Urinary frequency, urgency, and pain or burning sensations during urination.
- Ejaculatory Pain: Discomfort or pain experienced during or after orgasm.
- Sexual Dysfunction: Potential erectile dysfunction or loss of libido.
Conventional Pharmacological Interventions for Prostatitis
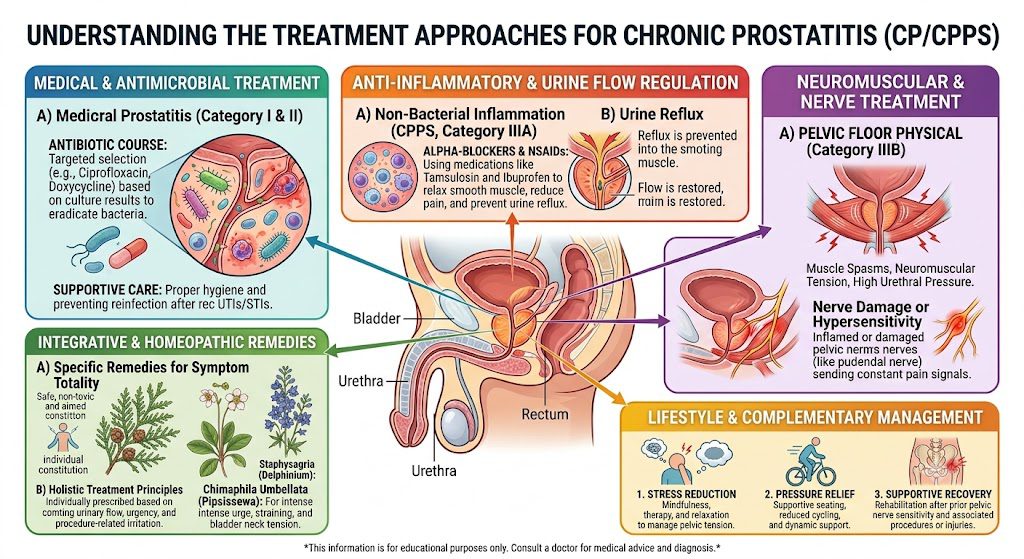
Oral antibiotics remain the mainstay and are widely described as the treatment of choice for chronic bacterial prostatitis, because prostate tissue penetration determines success; you should expect a prolonged regimen rather than a short course, with many clinicians aiming for a four- to six-week initial therapy as a practical benchmark.
Fluoroquinolones are often chosen for their excellent tissue penetration, with ciprofloxacin and levofloxacin as common first-line treatments for prostate infection; if culture results show resistance, treatment is adjusted based on susceptibility testing instead of continuing the same agent.
If you cannot tolerate fluoroquinolones or if pathogens show resistance, alternative antimicrobials such as trimethoprim-sulfamethoxazole or doxycycline are used, with treatment tailored to the identified organism and patient factors like allergy history and concurrent medications.
Standard Antibiotic Protocols
Initial empiric therapy is often started while you await culture and sensitivity results, and clinicians typically collect a urine culture plus post-prostatic massage specimens when possible, so definitive therapy can be targeted once findings arrive, usually within 48 to 72 hours.
Dosage and duration depend on the clinical picture; you may be prescribed a multi-week regimen for chronic presentations, and providers commonly reassess at set intervals to monitor symptom response and tolerability, especially in older patients or those with renal impairment.
Monitoring during and after therapy includes symptom scores, repeat urine cultures if symptoms persist, and assessment for adverse effects, so you should plan a follow-up visit at therapy completion and again if symptoms recur within weeks of stopping antibiotics.
Managing Persistent Bacterial Strains
Persistent organisms often indicate biofilm formation or intracellular reservoirs, and if you have recurrent infection despite standard therapy, specialists may recommend extended antibiotic courses lasting more than six weeks or combination regimens based on laboratory susceptibility testing.
When repeat cultures identify the same pathogen, you and your clinician should consider targeted strategies such as rotating antibiotic classes or using agents with proven intracellular activity, with decisions informed by culture history and prior treatment responses.
Referral to a urologist is appropriate for refractory cases, and you may be evaluated for structural contributors like prostatic calculi or obstruction, with surgical options such as drainage or transurethral intervention reserved for select, well-documented scenarios.
Longer-term management can include periodic surveillance cultures and coordinated care between your primary clinician and urology, and in practice many patients who fail initial outpatient regimens improve after multidisciplinary review and tailored extended therapy.
Holistic and Non-Antibiotic Healing Strategies for Chronic Prostate Infection
How to cure prostate infection without antibiotics: Natural treatment for prostate infection can begin with a structured plan discussed with your clinician, combining pelvic-floor physiotherapy, targeted phytotherapy such as saw palmetto, quercetin, and pygeum, and symptom-focused self-care. You should prioritize interventions that reduce pelvic tension and inflammation, rule out bacterial infection with appropriate testing, and consider pharmacy-formulated botanical combinations like saw palmetto, quercetin, and pygeum.
Pelvic-floor approaches address myofascial trigger points and neuromuscular coordination through biofeedback and manual release, and you should work with a therapist who provides hands-on sessions plus daily relaxation exercises to break the pain-tension cycle, often delivered as weekly clinic visits with prescribed home practice.
Lifestyle adjustments target bladder and prostate irritants, so you should increase plain-fluid intake, limit caffeine and alcohol, use warm sitz baths to reduce perineal discomfort, and practice pelvic relaxation techniques after bowel movements to lower symptom flares.
Integrative Recovery Models
Team-based care pairs urology oversight with pelvic physiotherapy, nutritional counseling, and mental-health support so you receive coordinated input on symptom drivers and treatment sequencing, for example, a primary-care referral that links you to a pelvic-floor physio within a multidisciplinary clinic.
Protocols frequently start with non-antibiotic measures when urine culture does not confirm bacterial prostatitis, and you should request baseline urine testing plus a symptom diary before committing to long-term antibiotics, while clinicians may trial phytotherapy alongside alpha-blockers where clinically appropriate.
Monitoring combines subjective tools and objective measures such as voiding diaries, pain scales, and repeat urine testing, and you should bring a short symptom diary to follow-up appointments so clinicians can adjust therapies based on real-world patterns.
Natural Wellness and Lifestyle Adjustments for Chronic Prostatitis Patients
Dietary tactics emphasize anti-inflammatory foods, reduced processed items, and attention to micronutrients, and you should consider adding omega-3-rich foods, probiotics, and zinc under medical supervision as part of a prostate infection natural treatment approach.
Exercise guidance favors gentle aerobic activity and pelvic-floor relaxation over heavy straining, so you should adopt nightly stretching or specific yoga poses that release pelvic tension and maintain moderate walking sessions most days to support circulation and recovery.
Sleep and stress management influence symptom perception and immune balance, and you should establish consistent bedtimes, practice breathing exercises before sleep, and use brief cognitive techniques to reduce pain-related hypervigilance during flare periods.
Supplementation often includes botanicals mentioned in discussions about curing prostate infection without antibiotics and natural treatments for prostate infection, so you should review saw palmetto, quercetin, pygeum, Cernilton pollen extract, and probiotics with your prescriber, as interactions and dosing vary.
Specialized Complementary Therapies for Chronic Prostatitis
 Traditional Acupuncture for Prostatic Health
Traditional Acupuncture for Prostatic Health
 Traditional Acupuncture for Prostatic Health
Traditional Acupuncture for Prostatic HealthUsing acupuncture for prostate infection and acupuncture for prostatitis, many clinicians target points on the lower abdomen and sacral region to modulate pelvic blood flow and nociceptive signaling, with the explicit aim of reducing local inflammation and pain. You should expect a diagnostic intake that maps urinary symptoms, pelvic pain, and systemic signs before point selection. Practitioners commonly suggest a course of weekly treatments, for example, eight to twelve sessions, and combine manual needling with adjuncts such as gentle moxibustion in some practice settings.
Clinical reports describe acupuncture for prostatitis most often as an adjunct to conventional care when antibiotics or alpha-blockers leave residual pain or urinary dysfunction, and you are typically counseled about realistic outcomes and monitoring. You may be offered electroacupuncture for persistent pelvic pain, which applies a mild current to selected needles to enhance neuromodulation. Many clinicians document symptom changes using a voiding diary and pain scale at baseline and after a defined treatment block such as a three-month review.
Expect sessions to include an initial intake, pulse and tongue assessment in traditional practice, and needle retention of around thirty to forty-five minutes, with sterile disposable needles used throughout. You should disclose anticoagulant use and any implanted devices, because those are relevant safety considerations. Reported adverse effects are generally limited to minor bruising or transient soreness, and informed consent with clear follow-up is standard in established clinics.

Homeopathic Protocols for Long-Term Relief in Patients with Chronic Prostatitis
Personalized homeopathy for prostate infection relies on a detailed case-taking that considers symptom patterns, emotional state, and past treatments, so you receive an individualized prescription rather than a one-size-fits-all product. Homeopaths select a single homeopathic remedy for chronic prostatitis based on the totality of signs and symptoms, then reassess the response at successive visits. You should expect potency adjustments and modifications if symptoms shift during the course of care.
When antibiotics have cleared an acute infection but pain or urinary complaints persist, a homeopathic remedy for chronic prostatitis may be proposed with the intention of long-term symptom control and fewer side effects than ongoing pharmacologic therapy. You will typically have follow-up consultations to evaluate changes in nocturia, urgency, and pelvic discomfort, with reviews every four to six weeks during the initial phase of care. Practitioners document responses using symptom diaries and periodic clinical review.
Practitioners caution that over-the-counter homeopathic remedies for prostatitis vary in composition and dosing, and you should consult a qualified homeopath before self-prescribing, particularly if you are taking other medications or supplements. Integrated care that coordinates homeopathy with your urologist can prevent conflicting advice and ensures monitoring for recurrent infection. Many clinics formalize care with a written treatment plan and monthly reviews to track progress.
Follow-up information for Homeopathic Protocols for Long-Term Relief emphasizes objective tracking, so you should use a symptom diary and an established symptom score (for example, a urinary symptom questionnaire) at baseline and again after a defined interval such as three months to assess benefit and determine whether the homeopathic remedy remains appropriate.
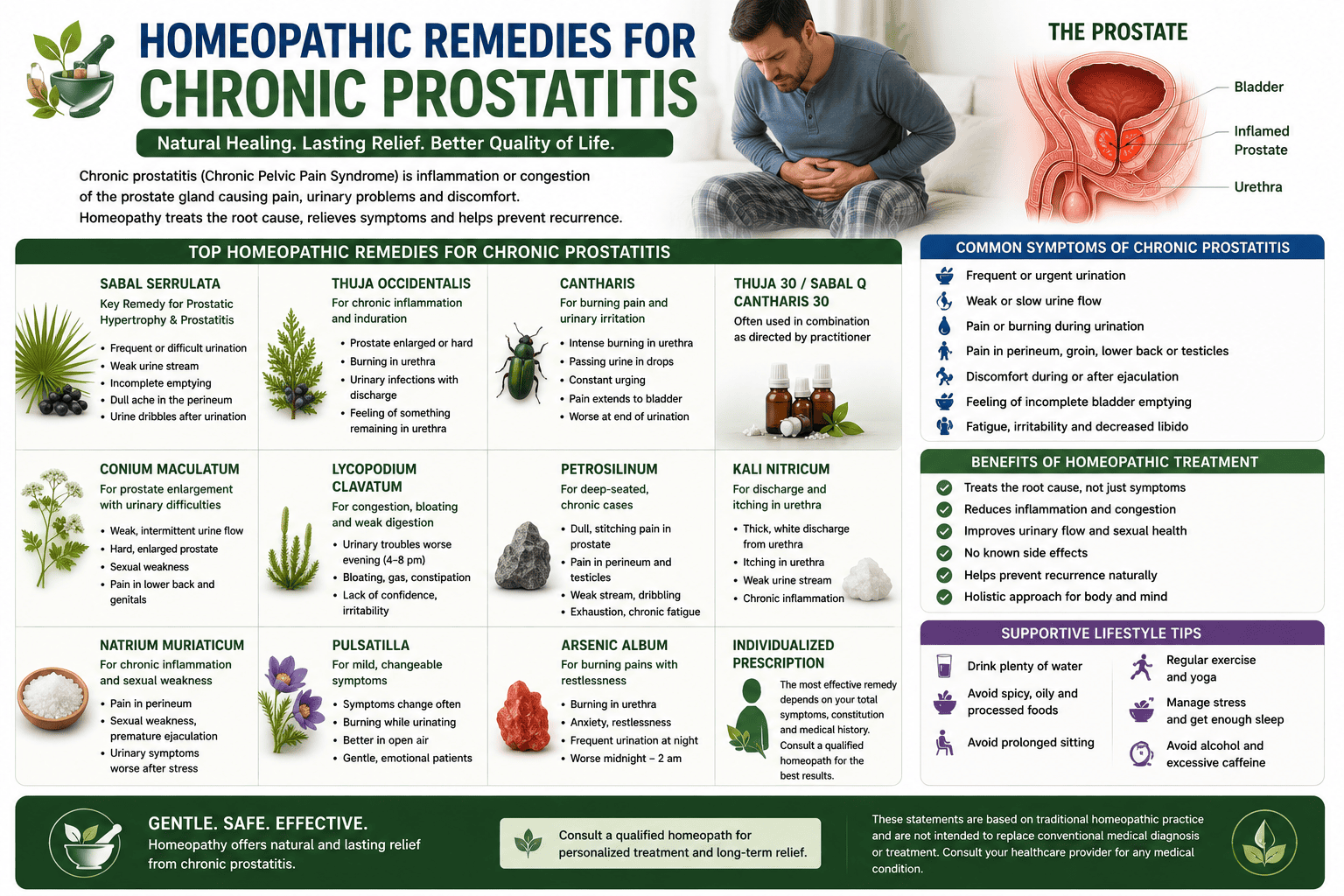
- Sabal serrulata: Indicated for frequent nightly urination, difficulty passing urine, and a cold sensation in the sexual organs.
- Thuja occidentalis: Frequently selected for persistent, sharp, or burning pelvic discomfort and general prostate inflammation.
- Conium maculatum: Used primarily when urine flow is weak or stops and starts or when there is a sensation of a hard, heavy ache in the pelvic floor.
- Lycopodium clavatum: Addressed when urine is very slow to emerge, accompanied by heavy pressure during or after urination, and gas or bloating.
- Staphysagria: Indicated for a constant burning sensation in the urethra even when urine is not flowing, often coupled with urinary retention.
- Chimaphila umbellata: Often given when a patient must strain significantly to initiate urination or experiences a sensation of sitting on a ball.
Final Words
You should consult a urologist to review prostatitis treatment options, including antibiotics for confirmed bacterial infections. Most clinicians acknowledge there is no single best cure for chronic prostatitis, so plans commonly combine medication, pelvic floor work, and pain-targeted strategies to address inflammation and pelvic pain.
Holistic measures such as pelvic floor physiotherapy, sitz baths, and dietary adjustments can reduce symptom burden for many men. Consider keeping a symptom diary to compare responses to sitz baths, physiotherapy sessions, or medications and identify specific triggers.
A multidisciplinary team, a urologist, a pelvic physiotherapist, and a pain specialist improve coordination of prostatitis treatment. You should expect ongoing management rather than a one-time cure for chronic cases, so schedule regular reviews and use symptom scores or voiding diaries to, for example, adjust the frequency of pelvic physiotherapy.
FAQ

Q: How do you get a prostate infection?
A: Bacterial prostate infections most often arise when bacteria ascend from the urethra into prostatic ducts, frequently after a urinary tract infection or instrumentation such as catheterization; urine reflux into the prostatic ducts can also introduce pathogens. Healthcare-associated procedures, for example, urinary catheter placement after surgery, are common precipitating events observed in hospital practice.
Q: Can a prostate infection be sexually transmitted?
A: Certain pathogens that cause acute prostatitis, including Neisseria gonorrhoeae and Chlamydia trachomatis, can be acquired through sexual contact and may involve the prostate, while the majority of bacterial prostatitis cases originate from enteric organisms like Escherichia coli rather than sexually transmitted routes. Testing for common sexually transmitted infections is routinely advised in sexually active men presenting with acute symptoms at sexual health or urology clinics.
Q: What is the most common cause of prostatitis?
A: In clinical settings the most frequent cause of bacterial prostatitis is infection with enteric Gram-negative bacteria. Escherichia coli was identified in many urine or prostatic secretion cultures; nonbacterial chronic pelvic pain syndrome occurs without a detectable infectious agent and represents a separate diagnostic category. Community urology practices commonly see urine cultures that grow E. coli.
Q: What symptoms should prompt evaluation for prostatitis, and how do they vary by type?
A: Acute bacterial prostatitis typically presents with high fever, chills, severe perineal pain, and obstructive urinary symptoms, including retention; chronic bacterial prostatitis often causes recurrent urinary tract infections, low-grade pelvic pain, and painful ejaculation, while chronic pelvic pain syndrome produces persistent pelvic discomfort with variable urinary and sexual dysfunction but no positive cultures. A markedly tender, swollen prostate on digital rectal exam frequently accompanies acute cases and often leads patients to seek emergency care for urinary retention.
Q: How is a prostate infection diagnosed in practice?
A: Diagnosis relies on clinical history and examination, urinalysis and urine culture, and targeted sampling such as pre- and post-prostatic massage urine cultures or expressed prostatic secretions when available; imaging with transrectal ultrasound or MRI is reserved for suspected abscesses or complicated cases. A positive culture from post-prostatic massage urine or expressed secretions is considered confirmatory in many urology clinics.
Q: What is the treatment of choice for chronic bacterial prostatitis?
A: Culture-directed antibiotic therapy that achieves adequate prostatic penetration is the mainstay, with commonly used regimens given for prolonged courses, often four to six weeks initially and extended if symptoms or cultures persist; alternatives and duration are adjusted based on sensitivity results and patient tolerance. Specialist follow-up is typical when a standard course of antibiotics fails or when procedures such as transrectal drainage are being considered.
Q: Is it possible to treat prostatitis without antibiotics? What holistic or complementary therapies have evidence to support them?
A: Nonbacterial chronic pelvic pain syndrome is mainly treated with multimodal, non-antibiotic approaches, including pelvic-floor physical therapy, alpha-blockers for urinary symptoms, anti-inflammatory agents for short-term symptom relief, thermal sitz baths, dietary changes (for example, reducing spicy foods and caffeine), and psychological strategies such as cognitive behavioral therapy for chronic pain. Acupuncture has shown promise in some small trials, while homeopathy lacks reliable evidence and should be discussed with a physician before use. A typical approach in specialty clinics is an eight- to-twelve-week trial of pelvic-floor physical therapy along with medications that target specific symptoms.
Natural and Holistic Treatments for Chronic Prostatitis in Philadelphia
Natural treatment for chronic prostatitis is effective, safe, and affordable. Using acupuncture and homeopathic remedies for prostate infection can save men from antibiotic therapy and other medical interventions. However, a medical doctor—not a naturopath or herbalist—should administer the natural treatment for prostatitis. It is imperative to perform a proper lab test and differential diagnosis to be sure that the enlargement, swelling, and pain of the prostate gland are benign and not a symptom of prostate cancer.
For an initial holistic evaluation with a medical doctor, Victor Tsan, contact our clinic and schedule your first appointment.