Peptic Ulcer Disease
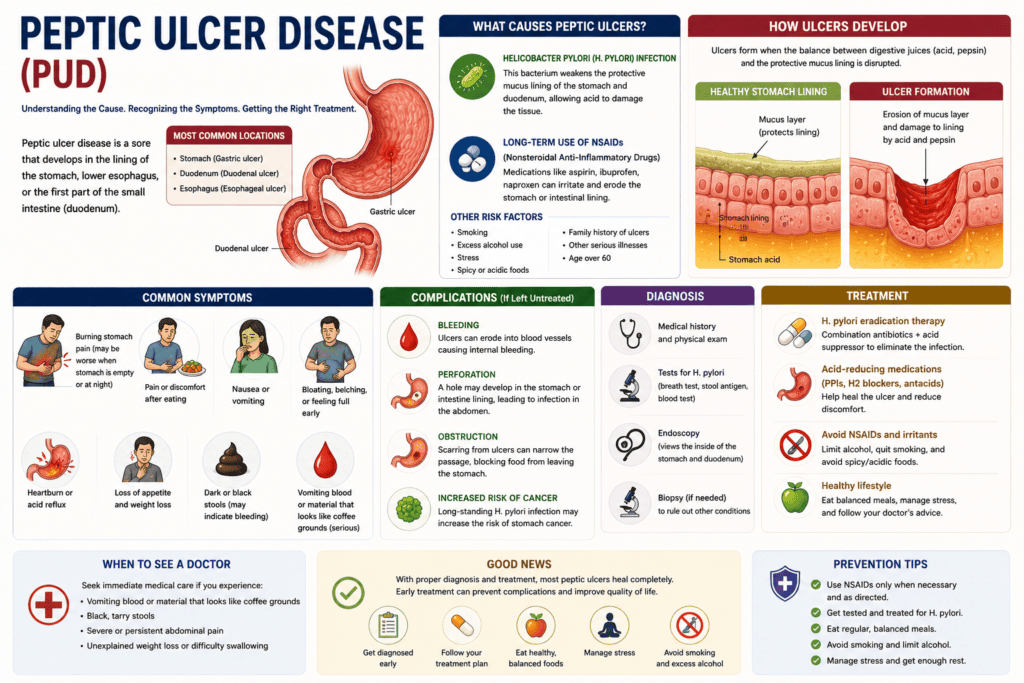
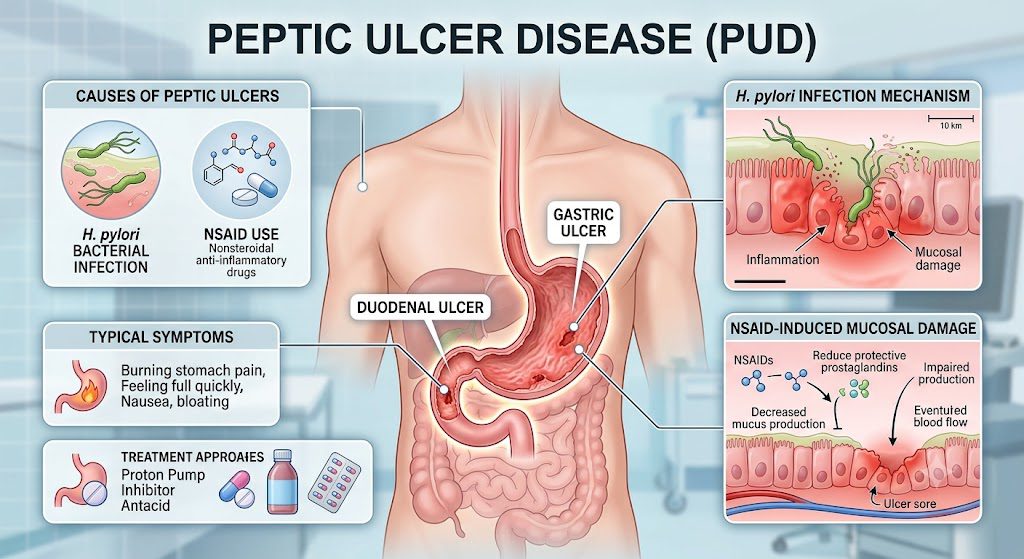
Peptic ulcer disease (PUD) causes open sores (ulcers) in the lining of your stomach or the upper part of your small intestine. It is primarily caused by H. pylori bacterial infection or overuse of NSAID pain relievers. The hallmark symptom is burning stomach pain, which can be diagnosed via endoscopy or breath tests. Helicobacter pylori infection or the use of nonsteroidal anti-inflammatory medicines (NSAIDs) are the main causes of peptic ulcer disease (PUD), which is characterized by mucosal abnormalities in the stomach or duodenum that extend into the muscularis mucosa.
 PUD is still a major cause of gastrointestinal morbidity and healthcare utilization, especially in older adults with high aspirin and NSAID requirements, even though the incidence has declined globally as a result of improved sanitation and H pylori eradication efforts. The “test and treat” approach for dyspepsia has been prioritized in management, with a focus on non-invasive testing using urea breath or monoclonal fecal antigen assays, as well as the use of vonoprazan-based regimens or optimized 14-day bismuth quadruple treatment to counteract growing antibiotic resistance. The prompt beginning of endoscopic evaluation to confirm diagnosis and rule out cancer depends on the prompt detection of warning characteristics, such as iron-deficiency anemia, overt bleeding, or unexpected weight loss.
PUD is still a major cause of gastrointestinal morbidity and healthcare utilization, especially in older adults with high aspirin and NSAID requirements, even though the incidence has declined globally as a result of improved sanitation and H pylori eradication efforts. The “test and treat” approach for dyspepsia has been prioritized in management, with a focus on non-invasive testing using urea breath or monoclonal fecal antigen assays, as well as the use of vonoprazan-based regimens or optimized 14-day bismuth quadruple treatment to counteract growing antibiotic resistance. The prompt beginning of endoscopic evaluation to confirm diagnosis and rule out cancer depends on the prompt detection of warning characteristics, such as iron-deficiency anemia, overt bleeding, or unexpected weight loss.
Key Takeaways:
- H. pylori bacteria and NSAIDs account for the majority of peptic ulcer cases. The bacterium Helicobacter pylori disrupts the protective mucosal lining of the stomach and duodenum, while nonsteroidal anti-inflammatory drugs inhibit prostaglandin synthesis, reducing the stomach’s natural defense mechanisms against acid damage.
- Burning epigastric pain that improves or worsens with food intake serves as the hallmark symptom. Duodenal ulcers typically cause pain two to three hours after meals or during the night, often relieved by eating, whereas gastric ulcers may produce discomfort immediately after food consumption.
- Proton pump inhibitors combined with antibiotic therapy form the standard medical treatment protocol. Triple or quadruple therapy regimens eradicate H. pylori infection while reducing gastric acid production, allowing the ulcer to heal within four to eight weeks in most patients.
- Dietary modifications support healing but do not replace medical treatment. Avoiding alcohol, caffeine, spicy foods, and acidic beverages reduces irritation to the gastric lining, while consuming smaller, more frequent meals helps manage symptoms during the recovery period.
- Stress reduction techniques complement conventional therapy by modulating the gut-brain axis. Chronic psychological stress increases gastric acid secretion and may impair mucosal blood flow, making mind-body practices like meditation and yoga valuable adjunctive approaches.
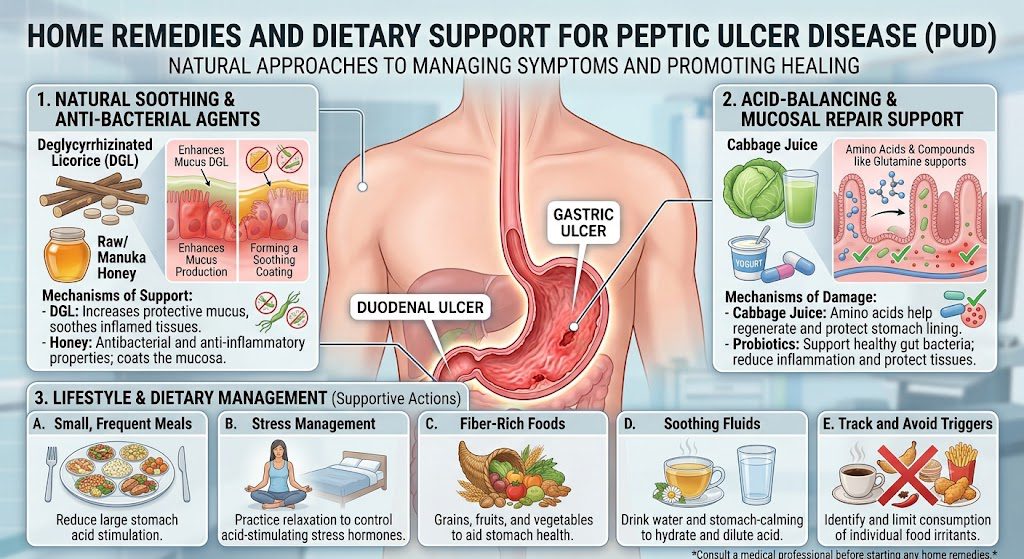
- Natural remedies including cabbage juice, licorice root, and probiotics show promise in clinical observations. These substances may enhance mucosal protection and support beneficial gut bacteria, though they should supplement rather than substitute evidence-based medical interventions.
- Untreated peptic ulcers can lead to life-threatening complications requiring emergency intervention. Perforation, bleeding, gastric outlet obstruction, and penetration into adjacent organs represent serious outcomes that necessitate immediate surgical consultation and intensive care management.
Clinical Presentation and Symptomatology of Peptic Ulcer Disease
Burning or gnawing epigastric pain represents the hallmark manifestation of peptic ulcer disease, typically localized between your navel and sternum. Your discomfort may intensify or subside in relation to meals, with gastric ulcers often worsening during or immediately after eating, while duodenal ulcers frequently improve with food intake but return two to three hours later. The pain can radiate to your back, particularly when posterior wall ulcers penetrate deeper tissue layers, and it may awaken you from sleep during the early morning hours when gastric acid secretion peaks naturally.
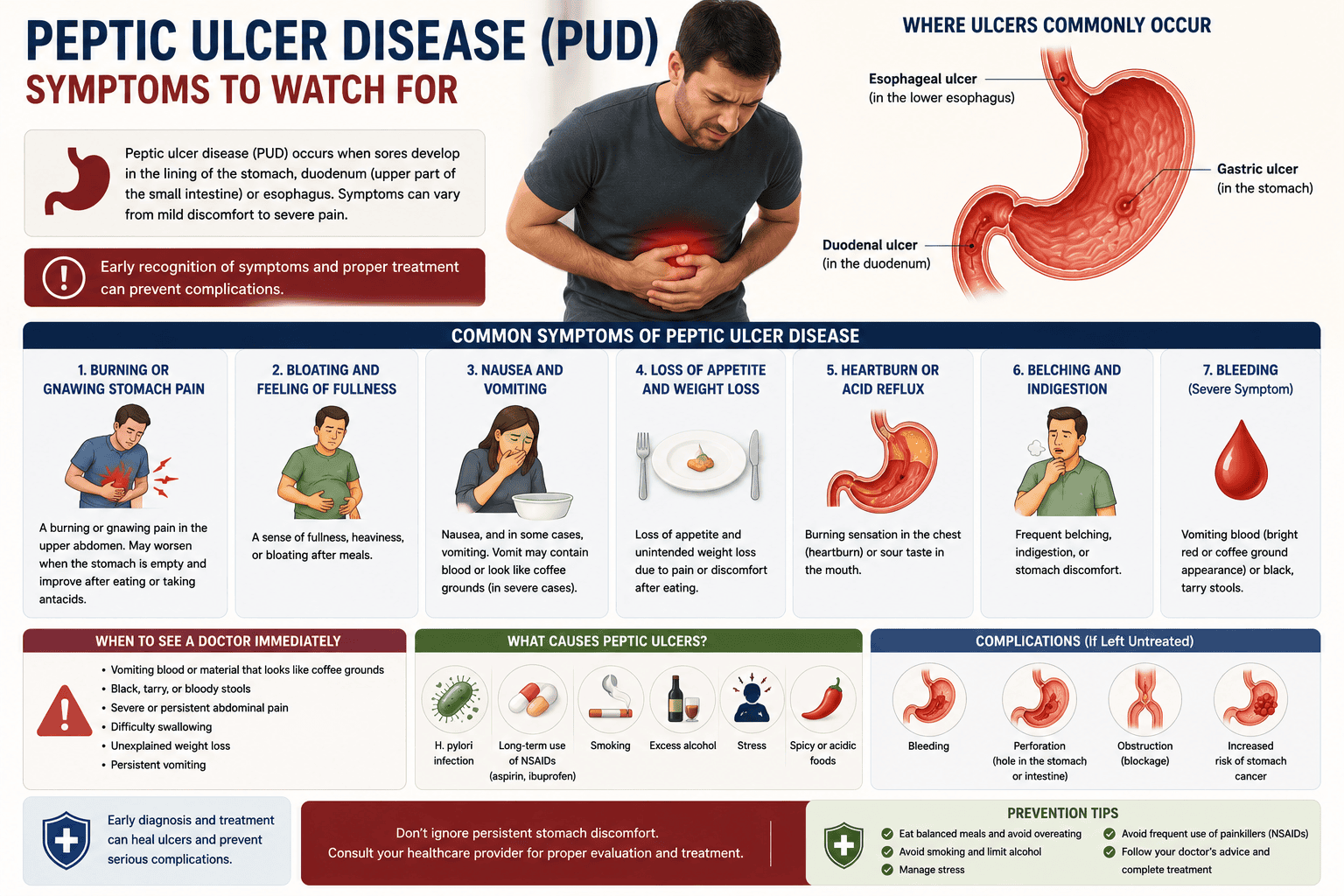
Nausea and early satiety commonly accompany the pain syndrome, making you feel uncomfortably full after consuming only small portions of food. Bloating and belching occur as your digestive system struggles with altered motility patterns caused by inflammation and mucosal damage. Some individuals experience heartburn and regurgitation similar to gastroesophageal reflux disease, which can complicate diagnostic differentiation. Your appetite may diminish significantly, leading to unintentional weight loss over weeks or months as you subconsciously avoid eating to prevent pain episodes.
Symptom patterns vary considerably based on ulcer location, size, and depth of penetration into the gastric or duodenal wall. Your experience may range from mild intermittent discomfort to severe persistent pain requiring immediate medical evaluation. Periods of active symptoms often alternate with asymptomatic intervals lasting weeks or months, particularly when H. pylori infection remains untreated or NSAID use continues intermittently. The episodic nature of these manifestations can delay diagnosis, as you may attribute temporary relief to dietary changes or over-the-counter antacids rather than seeking professional assessment.
Identifying common abdominal pain patterns
Duodenal ulcers produce a characteristic rhythmic pain pattern that follows a predictable cycle throughout your day. Your discomfort typically emerges two to five hours after meals when stomach contents have emptied and concentrated gastric acid contacts the exposed duodenal mucosa. This hunger pain often awakens you between midnight and 3 a.m., prompting you to seek relief through eating or drinking milk, which temporarily buffers the acid environment. The pain-food-relief pattern creates a distinctive clinical signature that helps differentiate duodenal from gastric pathology.
Gastric ulcers generate pain with an inverse relationship to food consumption, worsening within thirty to sixty minutes after eating as your stomach distends and acid production increases. You may develop food aversion as meals consistently trigger discomfort rather than providing relief, leading to progressive weight loss and nutritional deficiencies. The pain localizes more precisely to your left upper quadrant or midepigastric region, sometimes creating a tender spot you can identify with a single finger. Antacids provide only partial, temporary relief compared to the more complete response seen with duodenal ulcers.
Pain intensity and character provide additional diagnostic clues about ulcer severity and potential complications. Sharp, sudden pain that persists without relief suggests perforation, while pain radiating straight through to your back indicates posterior penetration into the pancreas or retroperitoneal space. Your pain may shift from dull and aching to severe and constant as the ulcer deepens through mucosal layers. Some individuals describe the sensation as burning; others, as gnawing or hunger-like, while a subset experiences only vague upper abdominal discomfort without clear localization or temporal patterns.
Recognizing secondary physical indicators and warning signs
Hematemesis, the vomiting of blood, signals active bleeding from your ulcer and requires immediate medical attention. You may vomit bright red blood when bleeding is brisk or dark brown material resembling coffee grounds when blood has been partially digested by gastric acid. Melena, characterized by black, tarry, foul-smelling stools, indicates that blood from your upper gastrointestinal tract has passed through your intestines and undergone bacterial degradation. Even small amounts of chronic blood loss can accumulate, causing iron-deficiency anemia with accompanying fatigue, pallor, shortness of breath, and lightheadedness during position changes.
Physical examination may reveal epigastric tenderness when your healthcare provider applies pressure to your upper abdomen, though this finding lacks
Etiology and Predisposing Risk Factors of Peptic Ulcer Disease
Understanding the root causes of peptic ulcer disease requires you to examine both infectious agents and environmental triggers that compromise your gastric mucosa’s protective mechanisms. Your digestive tract maintains a delicate balance between aggressive factors (acid and pepsin) and defensive elements (mucus, bicarbonate, and blood flow), and disruption of this equilibrium creates conditions for ulcer formation. The development of these lesions involves multiple pathways, ranging from bacterial colonization to medication-induced mucosal injury.
Several distinct factors elevate your susceptibility to developing peptic ulcers throughout your lifetime. Your exposure to certain bacteria, particularly Helicobacter pylori, represents the most common infectious cause worldwide. Beyond microbial influences, your medication choices and lifestyle habits play significant roles in determining ulcer risk:
- Chronic use of nonsteroidal anti-inflammatory drugs (NSAIDs), including aspirin
- Tobacco smoking, which impairs healing and increases acid secretion
- Excessive alcohol consumption that erodes mucosal barriers
- Psychological stress and irregular eating patterns
- Family history suggesting genetic predisposition
Your individual risk profile emerges from the interplay between these variables, with some factors exerting stronger influence than others. Knowing these contributors allows you to identify modifiable behaviors and seek appropriate medical evaluation when symptoms arise.
The role of H. pylori and the primary cause of mucosal damage
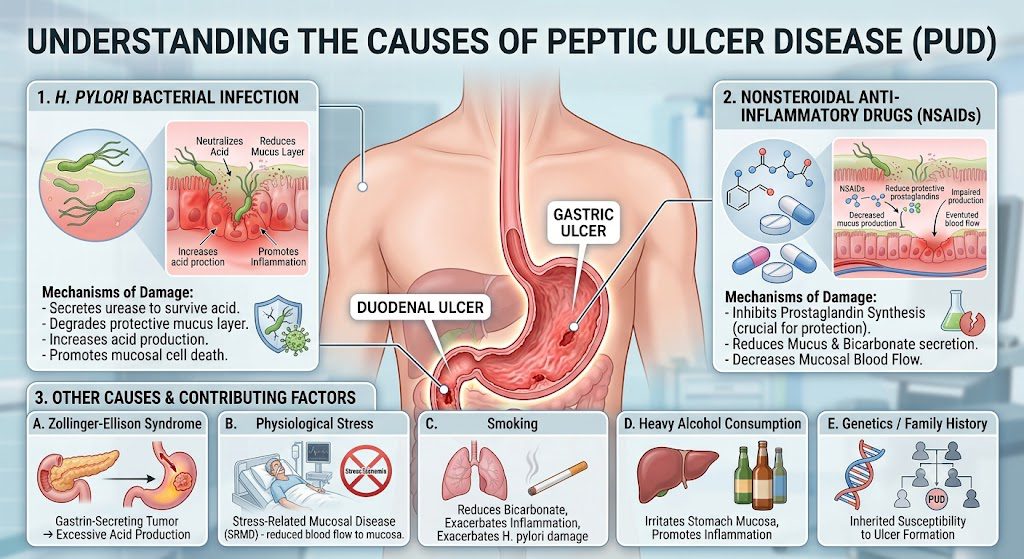
Helicobacter pylori infection stands as the leading cause of peptic ulcer disease globally, accounting for the majority of duodenal and gastric ulcers in your digestive system. This spiral-shaped bacterium colonizes your stomach lining and produces urease enzymes that neutralize gastric acid in its immediate environment, creating a survival niche in the hostile acidic environment. The organism’s presence triggers chronic inflammation that weakens your mucosal defenses over decades, though not everyone infected develops ulcers.
Your immune response to H. pylori paradoxically contributes to tissue damage rather than providing complete protection. The bacterium avoids being eliminated by using different methods, such as changing its surface antigens and living under your protective mucus layer. This persistent infection causes ongoing inflammation with cytokines and immune cells, which gradually damage the epithelial layer. The pathogen also disrupts your gastric physiology by interfering with regulatory hormones that control acid secretion.
Transmission of H. pylori typically occurs during childhood through person-to-person contact, often within families sharing close living quarters and meals. Your socioeconomic conditions during early life significantly influence acquisition rates, with crowded housing and limited sanitation increasing exposure risk. Once established, the infection persists indefinitely unless you undergo specific antibiotic eradication therapy, maintaining a reservoir for ulcer development throughout your adult years.
Analyzing pharmaceutical, genetic, and lifestyle risk factors
Nonsteroidal anti-inflammatory drugs are the second most common cause of peptic ulcers after H. pylori, and they can directly injure your gastric mucosa in several ways. These medications inhibit cyclooxygenase enzymes that produce prostaglandins, compounds crucial for maintaining your stomach’s protective mucus layer and adequate mucosal blood flow. Your risk escalates with higher doses, prolonged duration of use, and advanced age, particularly if you take these drugs without food or gastroprotective agents.
- Selective COX-2 inhibitors carry lower but still measurable ulcer risk
- Corticosteroids amplify NSAID-related complications when taken concurrently
- Anticoagulants and antiplatelet agents increase bleeding risk from existing ulcers
- Bisphosphonates may cause esophageal and gastric irritation
Genetic factors influence your susceptibility through variations in immune response genes, inflammatory mediators, and acid secretion patterns. Blood type O individuals demonstrate higher peptic ulcer rates compared to other ABO groups, though the mechanism remains incompletely understood. Your inherited traits also determine how efficiently you metabolize certain medications and
Conventional Medical Interventions and Pharmacotherapy for Peptic Ulcer Disease
Your healthcare provider will typically prescribe a combination of medications designed to reduce stomach acid production, eliminate bacterial infection, and protect the gastric lining. Proton pump inhibitors (PPIs), like omeprazole, lansoprazole, and esomeprazole, are the main treatment for peptic ulcer disease because they block the enzyme system that causes acid secretion in the stomach’s parietal cells. H2-receptor antagonists, such as ranitidine and famotidine, provide another way to reduce stomach acid, but they are usually less effective than PPIs. Antacids containing aluminum hydroxide, magnesium hydroxide, or calcium carbonate provide rapid but temporary relief by neutralizing existing stomach acid rather than preventing its production.
Treatment duration varies depending on ulcer severity and location, with most peptic ulcer medication regimens lasting between four and eight weeks for duodenal ulcers and up to twelve weeks for gastric ulcers. Your physician will assess healing progress through follow-up endoscopy, particularly for gastric ulcers where malignancy must be ruled out. Bismuth subsalicylate has two roles in treating peptic ulcers: it coats the ulcer crater and kills H. pylori. Sucralfate acts as a protective barrier, binding to ulcer sites and creating a physical shield against acid and pepsin damage.
Surgical intervention becomes necessary when medical management fails or complications arise, including perforation, obstruction, or uncontrolled bleeding. Procedures range from simple oversewing of perforations to partial gastrectomy in refractory cases. Your doctor may recommend vagotomy to reduce acid production by cutting the vagus nerve branches that stimulate gastric secretion. Emergency surgery carries higher mortality rates compared to elective procedures, making early diagnosis and appropriate peptic ulcer disease treatments crucial for preventing life-threatening complications.
Standard pharmacological protocols for acid suppression
Proton pump inhibitors represent the most effective class of acid-suppressing medications available for peptic ulcer disease treatments, achieving healing rates exceeding 90% when used consistently. Your body requires these medications to be taken 30 to 60 minutes before meals for optimal effectiveness, as they work best when the proton pumps are actively secreting acid. Omeprazole at 20-40 mg daily, pantoprazole at 40 mg daily, and lansoprazole at 30 mg daily constitute standard dosing regimens, though your physician may adjust these based on ulcer location and severity. Long-term PPI use beyond eight weeks requires careful monitoring due to potential side effects including vitamin B12 deficiency, increased fracture risk, and possible kidney disease.
H2-receptor antagonists block histamine receptors on gastric parietal cells, reducing acid secretion by about 70%, while PPIs reduce it by 90-95%. Famotidine at 40 mg once daily or 20 mg twice daily provides effective acid suppression for many patients, particularly those with milder disease or NSAID-induced ulcers. Ranitidine was previously a popular choice at 150 mg twice daily until its withdrawal from markets due to contamination concerns. These medications offer faster onset of action than PPIs but require more frequent dosing and may develop tachyphylaxis with prolonged use.
Antacids provide immediate symptomatic relief by chemically neutralizing hydrochloric acid already present in the stomach, raising gastric pH within minutes of administration. Calcium carbonate provides the strongest acid-neutralizing capacity at 500-1000 mg as needed, but it can cause constipation and rebound acid hypersecretion. Aluminum-magnesium combinations balance the constipating effects of aluminum with the laxative properties of magnesium, making them better tolerated for regular use. Your peptic ulcer medication schedule should separate antacid administration from other drugs by at least two hours, as they can interfere with the absorption of antibiotics, iron supplements, and certain cardiac medications.
Targeted medication for bacterial eradication and healing
Helicobacter pylori eradication requires triple or quadruple therapy regimens that combine antibiotics with acid suppressors, achieving cure rates of 80-90%.
Nutritional Strategies and Home-Based Care for Peptic Ulcer Disease
Your dietary choices play a fundamental role in managing peptic ulcer disease and promoting mucosal healing. Evidence-based nutritional strategies have largely replaced the traditional bland diet approach, focusing on reducing gastric irritation while supporting tissue repair. You should prioritize foods that buffer stomach acid and avoid those that stimulate excessive acid production or directly damage the gastric lining. Small, frequent meals throughout the day help maintain stable pH levels in your stomach, preventing the acid spikes that can exacerbate ulcer symptoms.
Certain foods require elimination or significant reduction in your daily intake when managing peptic ulcers. Spicy foods, caffeine, alcohol, and carbonated beverages can all increase gastric acid secretion and delay healing. You’ll find that citrus fruits and tomato-based products may trigger discomfort due to their high acidity. Processed meats and fried foods should be limited, as their high fat content slows gastric emptying and prolongs acid exposure to ulcerated tissue.
Hydration remains necessary for ulcer management, though you should be selective about your beverage choices. Water serves as the optimal choice for maintaining adequate fluid intake without stimulating acid production. Herbal teas, particularly chamomile and licorice root preparations, can provide soothing effects on the gastric mucosa. You must avoid drinking large quantities of fluids with meals, as the excess dilutes digestive enzymes and may prolong digestion time.
Evidence-based dietary modifications for gut health
Probiotic-rich foods offer significant benefits for your digestive system by restoring healthy bacterial balance and supporting mucosal defense mechanisms. Yogurt containing live cultures, kefir, and fermented vegetables like sauerkraut introduces beneficial bacteria that compete with H. pylori colonization. You can incorporate these foods daily to enhance your gut microbiome diversity and strengthen the protective mucus layer that shields your stomach lining from acid damage.
Flavonoid-containing foods demonstrate protective properties against peptic ulcer formation and progression. Apples, celery, cranberries, and onions all contain these plant compounds that inhibit H. pylori growth and reduce inflammation. You should include various colorful vegetables in your meals, as different pigments indicate distinct flavonoid profiles. Cruciferous vegetables such as broccoli and cabbage contain sulforaphane, a compound that has shown antimicrobial activity against the bacteria responsible for most ulcers.
Soluble fiber sources create a protective coating along your gastrointestinal tract while promoting regular bowel movements. Oatmeal, barley, and psyllium husk form a gel-like substance when mixed with stomach fluids, which can buffer acid and protect exposed ulcer craters. You’ll benefit from consuming these foods during breakfast or as part of your evening meal. Bananas offer a dual benefit, providing both soluble fiber and compounds that stimulate mucus production in your stomach lining.
Effective home remedies for management of symptoms of peptic ulcer disease
Cabbage juice has been used for decades as a traditional remedy for peptic ulcers, with some clinical observations supporting its effectiveness. The juice contains vitamin U (S-methylmethionine), which may accelerate healing of the gastric mucosa. You can prepare fresh cabbage juice by blending raw cabbage with water and consuming approximately one quart daily in divided doses. The taste can be challenging, so mixing it with carrot or celery juice improves palatability without diminishing its therapeutic potential.
Honey possesses natural antibacterial properties that may help combat H. pylori while coating and soothing irritated stomach tissue. Raw, unprocessed honey contains enzymes and compounds that support tissue regeneration. Take one to two tablespoons of honey on an empty stomach, preferably in the morning and before bedtime. Manuka honey from New Zealand has demonstrated particularly strong antibacterial activity in laboratory studies, though any raw honey variety can provide benefits.
Aloe vera juice offers anti-inflammatory and healing properties when consumed internally for ulcer management. The gel from this plant contains polysaccharides that stimulate mucus secretion and enhance the stomach’s protective barrier. You can drink one-quarter cup of aloe vera juice before meals to reduce acid.
Integrative Therapies and Holistic Modalities Utilizing Acupuncture for Peptic Ulcer Disease
Acupuncture offers you a time-tested approach to managing peptic ulcer disease by targeting specific meridian points that influence gastric acid secretion and mucosal healing. Traditional Chinese Medicine practitioners typically focus on points along the stomach and spleen meridians, particularly ST36 (Zusanli) and PC6 (Neiguan), which have been shown to reduce gastric hypersecretion and improve digestive harmony. Your treatment protocol may involve weekly sessions over several months, with practitioners inserting fine needles at depths ranging from 0.5 to 1.5 inches depending on the anatomical location.
Clinical applications of acupuncture for peptic ulcer disease extend beyond symptom relief to address underlying imbalances in your body’s energy flow. Practitioners assess your tongue coating, pulse quality, and overall constitution to create individualized treatment plans that may combine body acupuncture with auricular (ear) points. Stimulation of these specific points seems to change vagal nerve activity and increase the production of protective prostaglandins in your gastric lining.
Sessions typically last between 20 and 40 minutes, during which you rest comfortably while the needles remain in place. Many patients report experiencing reduced epigastric pain, decreased acid reflux, and improved appetite within four to six treatment sessions. Your acupuncturist may also incorporate moxibustion (the burning of the mugwort herb near acupuncture points) to warm and strengthen your digestive system, particularly if you present with cold-type symptoms such as a preference for warm beverages and foods.
Principles of homeopathy and specific homeopathic remedy applications for peptic ulcer disease
Homeopathy treats peptic ulcer disease based on the principle of “like cures like,” which means that substances causing symptoms in healthy people are used in very diluted forms to treat similar symptoms in people with ulcers. Your homeopathic practitioner will conduct an extensive consultation examining not only your physical symptoms but also your emotional state, food preferences, and response to environmental factors. This comprehensive assessment determines which constitutional remedy matches your unique symptom picture rather than simply addressing the ulcer diagnosis itself.
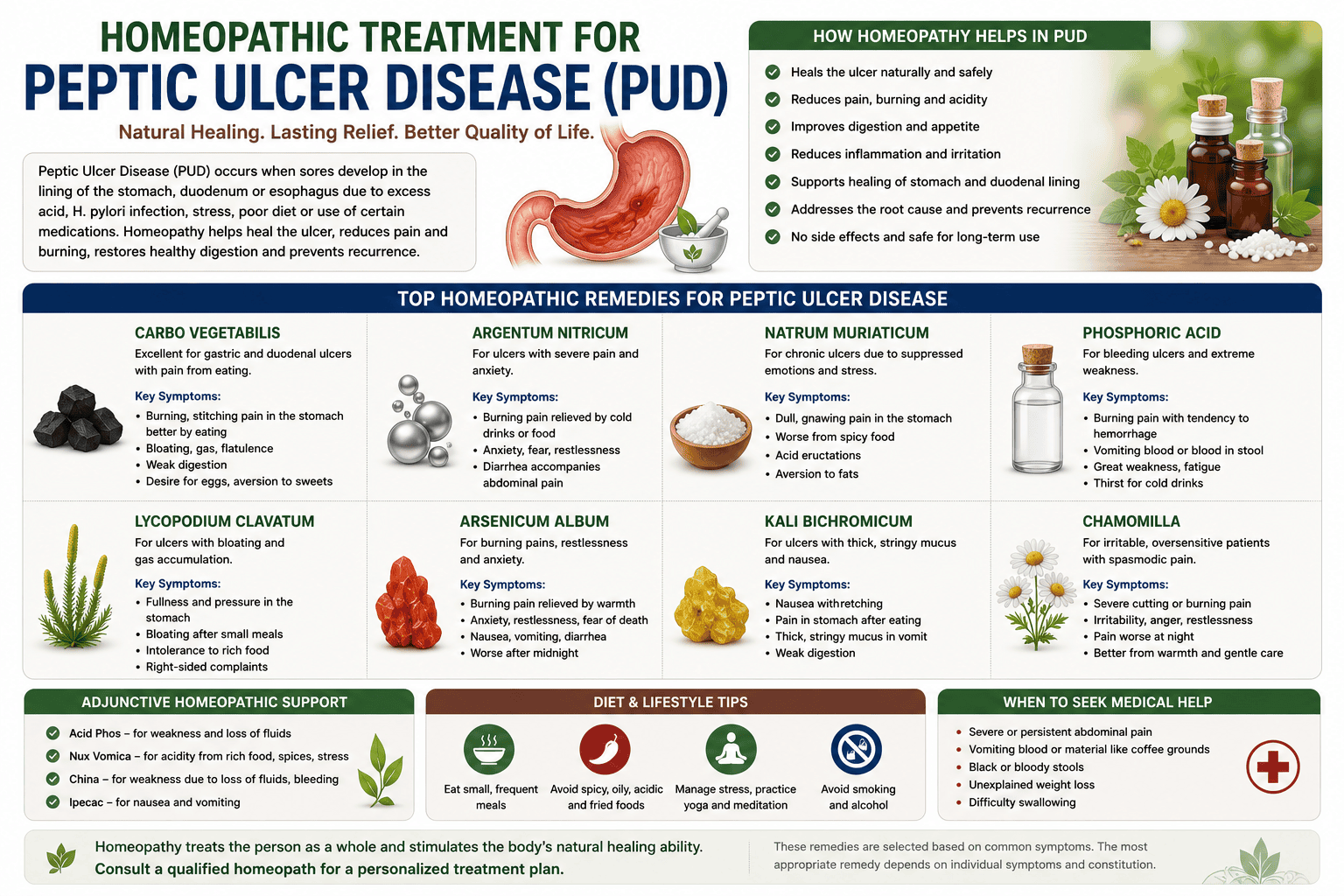
Several homeopathic remedies have established track records in treating peptic ulcer symptoms, each corresponding to distinct symptom patterns you might experience. Arsenicum album suits you if your ulcer pain improves with warm applications and you experience burning sensations coupled with anxiety and restlessness. Nux vomica becomes the remedy of choice when your symptoms worsen after consuming coffee, alcohol, or spicy foods, and you tend toward irritability and digestive complaints related to stress or overindulgence.
Phosphorus serves as an appropriate remedy when you experience burning stomach pain relieved by cold drinks, though the relief proves temporary, and you may notice a tendency toward bleeding or vomiting. Argentum nitricum addresses your symptoms if you suffer from intense anxiety, flatulence, and a strong craving for sweets that paradoxically worsen your condition. Lycopodium benefits you when bloating and gas accompany your ulcer symptoms, particularly if discomfort intensifies between 4 and 8 PM and you feel better after warm beverages.
In homeopathic treatment, your practitioner must choose the right potency and dosing frequency, as remedies usually come in dilutions from 6C for acute symptom management to 200C or higher for constitutional treatment. Your response to the initial remedy guides subsequent prescriptions, with practitioners monitoring changes in pain intensity, digestive function, and overall well-being. The individualized nature of homeopathic prescribing means two patients with identical endoscopic findings may receive entirely different remedies based on their unique presentations and constitutional characteristics.
Final Words
Your approach to managing peptic ulcer disease requires a comprehensive strategy that addresses both immediate symptoms and underlying causes. The best way to heal is to combine conventional pharmacotherapy (proton pump inhibitors, H2 receptor antagonists, and H. pylori eradication protocols) with evidence-based holistic interventions. Dietary modifications that emphasize anti-inflammatory foods, stress reduction techniques such as meditation and yoga, and targeted supplementation with probiotics and zinc carnosine work together with medical treatments to restore mucosal integrity and prevent recurrence.
The integration of medical and holistic modalities allows you to address multiple dimensions of peptic ulcer disease simultaneously. While medications control acid secretion and eliminate bacterial infections, nutritional strategies help repair tissue, herbal remedies like deglycyrrhizinated licorice protect the mucosa, and mind-body practices reduce the physiological effects of stress on gastric function. This multifaceted approach recognizes that peptic ulcers develop through complex interactions between infectious agents, lifestyle factors, and individual susceptibility patterns.
Your success in managing this condition depends on consistent adherence to treatment protocols and ongoing communication with healthcare providers. Regular monitoring ensures that healing progresses appropriately and allows for adjustments based on your response to therapy. Evidence shows that patients who use integrative care, combining conventional medicine with holistic interventions, often have faster symptom resolution, better quality of life, and lower rates of ulcer recurrence than those who rely only on pharmaceutical approaches.
FAQ

Q: What is the difference between a peptic ulcer and a gastric ulcer?
A: A peptic ulcer is the broader medical term for open sores that develop in the lining of the digestive tract, while a gastric ulcer specifically refers to ulcers located in the stomach. Peptic ulcers include both gastric ulcers and duodenal ulcers (found in the upper portion of the small intestine). The distinction matters because gastric ulcers often cause pain during or immediately after eating, whereas duodenal ulcers typically produce discomfort two to three hours after meals or during the night. Both types share common causes like H. pylori infection and NSAID use, but gastric ulcers may require different monitoring protocols due to a slightly higher risk of malignancy in rare cases.
Q: What are the most common symptoms of peptic ulcer disease?
A: Burning stomach pain represents the hallmark symptom of peptic ulcer disease, typically felt between the breastbone and navel. This discomfort often improves temporarily after eating or taking antacids, then returns several hours later. Patients frequently report bloating, belching, and a feeling of fullness after consuming small amounts of food. Nausea and vomiting may occur, particularly with gastric ulcers. Some people experience unintended weight loss due to eating avoidance triggered by meal-related pain. Dark or tarry stools indicate bleeding ulcers and require immediate medical attention, as do symptoms like vomiting blood or material resembling coffee grounds. About one in four people with peptic ulcers experience no symptoms at all, discovering the condition only when complications arise.
Q: What is the primary cause of peptic ulcers today?
A: Helicobacter pylori bacterial infection accounts for approximately 60-70% of peptic ulcers worldwide, making it the leading cause. This spiral-shaped bacterium damages the protective mucous coating of the stomach and duodenum, allowing acid to create ulceration. Long-term use of nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen, aspirin, and naproxen represents the second major cause, responsible for roughly 20-30% of cases. These medications inhibit prostaglandin production, which normally helps maintain the stomach’s protective mucus layer. The combination of H. pylori infection and NSAID use dramatically increases ulcer risk. Smoking, excessive alcohol consumption, and severe physiological stress from critical illness or major surgery contribute to a smaller percentage of cases, though these factors often act as aggravating influences rather than primary causes.
Q: What medications are typically prescribed for peptic ulcer treatment?
A: Proton pump inhibitors (PPIs) such as omeprazole, lansoprazole, and pantoprazole form the cornerstone of peptic ulcer pharmacotherapy by reducing stomach acid production for six to eight weeks. H. pylori-positive patients receive triple or quadruple therapy that combines a PPI with two or three antibiotics (commonly clarithromycin, amoxicillin, or metronidazole) for 10-14 days to eradicate the infection. H2-receptor antagonists like ranitidine or famotidine offer an alternative acid-suppression approach, though they work less powerfully than PPIs. Patients taking NSAIDs may receive misoprostol or high-dose PPIs as protective agents if they must continue these medications. Bismuth subsalicylate provides both protective coating and mild antibacterial effects. Antacids containing calcium carbonate or magnesium hydroxide offer rapid but temporary symptom relief without promoting healing.
Q: What dietary changes help manage peptic ulcer disease?
A: Eating smaller, more frequent meals throughout the day prevents excessive stomach acid production triggered by large portions and long fasting periods. Foods rich in flavonoids—including apples, berries, celery, and green tea—may help inhibit H. pylori growth and reduce inflammation. Fermented foods like yogurt, kefir, and sauerkraut containing probiotics support beneficial gut bacteria that compete with H. pylori.
Holistic Treatment for Peptic Ulcer Disease in Philadelphia
There are many different options if you choose a natural treatment for peptic ulcers. You just need to see which one works for you, and you will be quite impressed with the value provided by most options listed above. Not only are they very healthy, but they will help you protect your stomach or heal any signs of ulcers naturally. Stay away from using too much of any compound, since even these peptic ulcer remedies can be problematic if you overdo it. Talking with a medical professional is important since you want to prevent any bad interactions with your current treatments. These natural treatments are extraordinary and work well for most people, so they are worth a try!
Philadelphia Holistic Clinic, the home of holistic medicine in Philadelphia, sits in the northeast of the City of Brotherly Love. The clinic quickly became the metro area’s leading acupuncture, homeopathy, and hypnotherapy center. Dr. Tsan, the clinic’s medical director, has over 40 years of academic and practical experience in internal medicine and naturopathy.
Victor Tsan, MD, an internationally recognized specialist in traditional Chinese medicine, classical homeopathy, and clinical hypnotherapy, graduated from the most famous medical schools in Europe, Asia, and the USA.
For your initial holistic evaluation by Victor Tsan, MD, contact our clinic at (267) 403-3085 or book it online.