Delirium
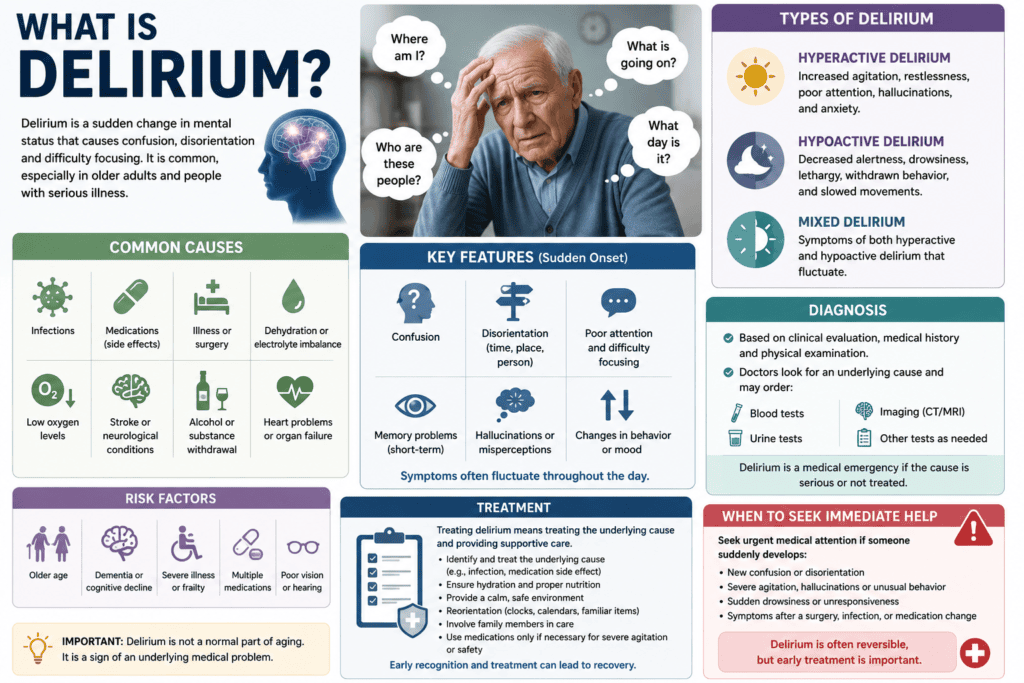
Delirium is a sudden, severe change in mental function that causes confusion, disorientation, and disrupted attention. It usually comes on quickly over a few hours or days and is often a treatable medical emergency.
A significant alteration in mental capacity is delirium. People become disoriented and oblivious to their surroundings as a result. This illness develops quickly. The onset of symptoms usually takes several hours or days.
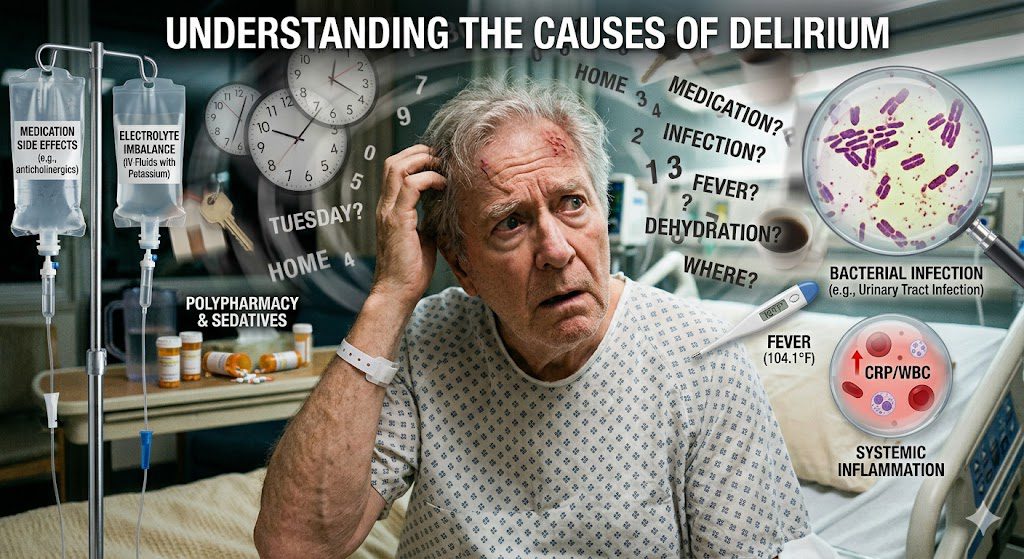
Delirium can be brought on by various medical issues, such as a severe or protracted illness. Lack of a vital nutrient, such as low salt levels, may be the cause of delirium. Certain medications, infections, surgeries, and substance use or withdrawal, including alcohol and other narcotics, can also result in delirium.
Key Takeaways:
- Delirium is an acute neurocognitive disorder characterized by a sudden onset of confusion, inattention, and fluctuating mental status, often mistaken for dementia despite key differences in progression and reversibility.
- A mid-sized SaaS firm managing employee health records observed that postoperative patients over age 70 accounted for nearly half of documented delirium cases, highlighting age and hospitalization as significant clinical markers.
- The condition arises from diverse etiologies, including infection, medication toxicity, metabolic imbalances, and trauma, with systemic inflammation and neurotransmitter disruption playing central roles in its development.
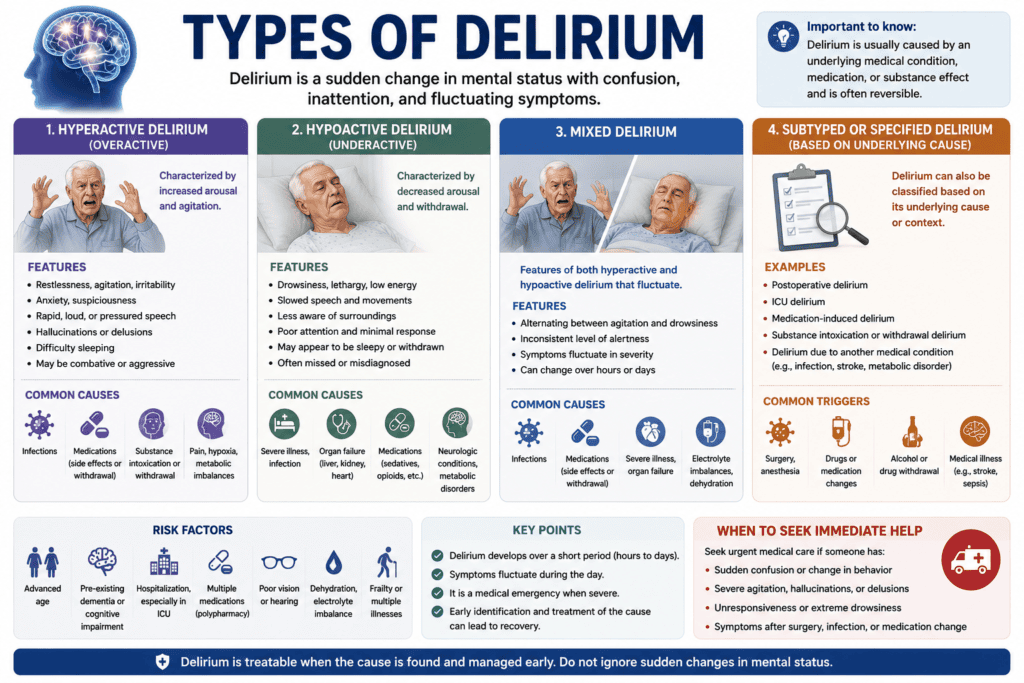
- Three primary subtypes—hyperactive, hypoactive, and mixed—present distinct clinical profiles, with hypoactive delirium frequently overlooked due to its subtle presentation of lethargy and withdrawal.
- Alcohol withdrawal can trigger a severe form known as delirium tremens, marked by autonomic instability, hallucinations, and a high mortality rate without prompt medical intervention.
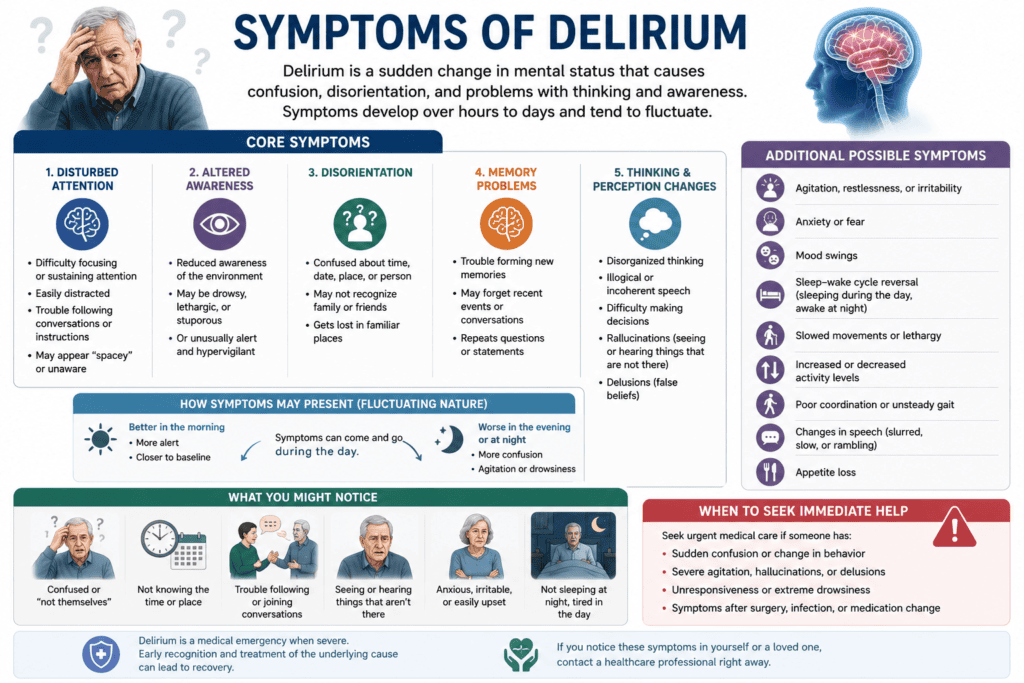
- Core symptoms such as disorganized thinking, altered sleep-wake cycles, and perceptual disturbances enable differentiation from chronic cognitive syndromes when assessed through standardized tools like the Confusion Assessment Method (CAM).
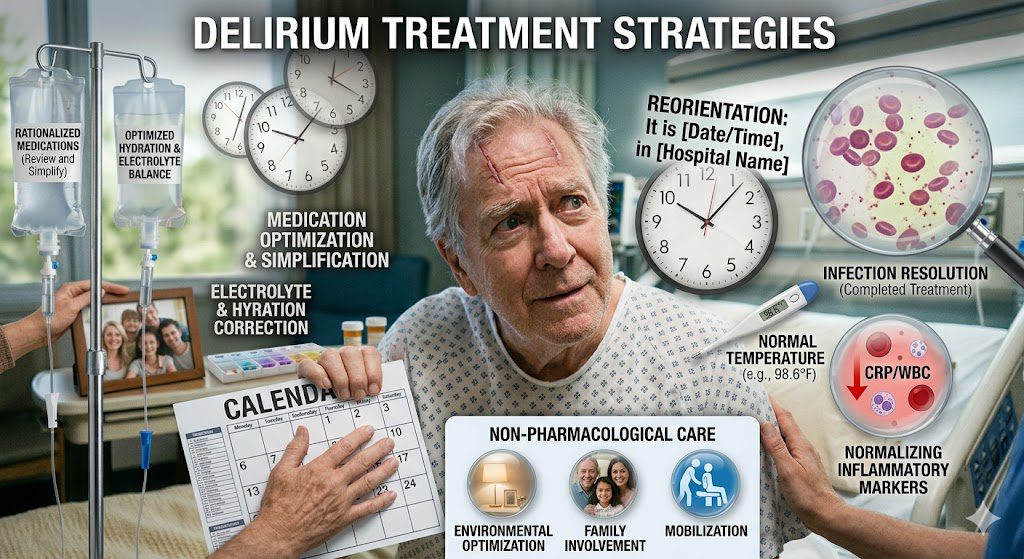
- Management prioritizes non-pharmacological strategies, including early mobilization, sleep hygiene, and orientation aids, with antipsychotics reserved for select cases involving extreme agitation or safety concerns.
Pathophysiology of Delirium and Differential Diagnosis
Neurological mechanisms of delirium and biological pathways
Disruption in neurotransmitter systems, particularly acetylcholine and dopamine, underpins the pathophysiology of delirium. A deficit in cholinergic activity impairs attention and memory, while excess dopamine contributes to agitation and hallucinations commonly seen in hyperactive subtypes. Neuroinflammation, often triggered by infection or surgery, activates microglia and releases cytokines that further disrupt neural circuits in vulnerable individuals. These changes predominantly affect the prefrontal cortex and thalamus, regions critical for executive function and arousal regulation. Metabolic disturbances, hypoxia, or drug toxicity can amplify this neurochemical imbalance, leading to the acute onset of cognitive dysfunction characteristic of delirium. The cumulative effect is a transient but severe breakdown in information processing across multiple brain networks.
Distinguishing acute delirium from chronic dementia
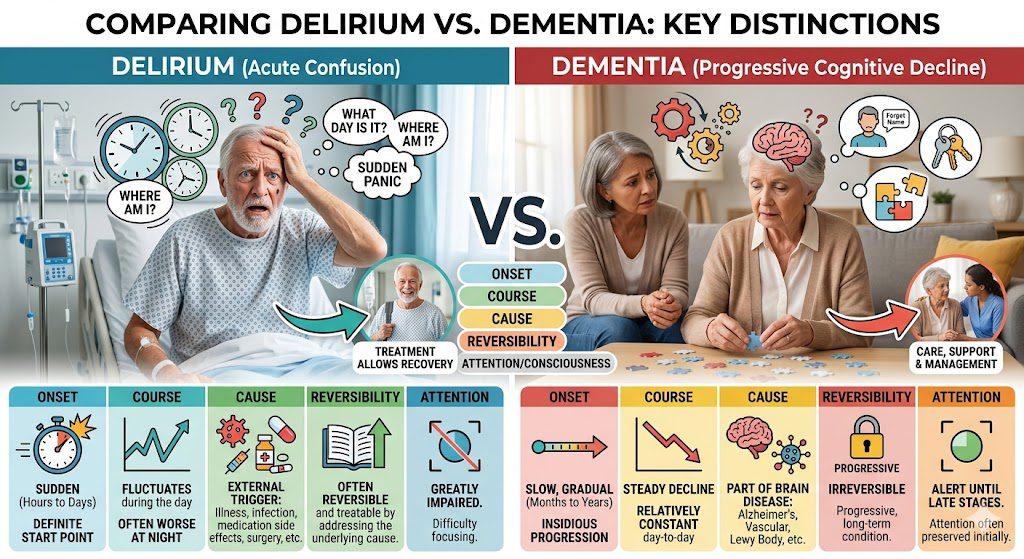
Onset timing provides the most immediate clue when differentiating delirium from dementia. Delirium emerges abruptly, often over hours to days, whereas dementia progresses gradually over months or years. You may observe fluctuating cognition throughout the day in delirium, with periods of lucidity interspersed with confusion, a pattern rarely seen in stable dementia. Attention deficits are more pronounced in delirium, particularly in tasks requiring sustained focus, such as serial sevens or name recall. A patient with Alzheimer’s disease might forget recent events but remain alert and oriented in the moment, while someone with delirium struggles to follow a simple conversation. Structural brain changes in dementia, visible on MRI as hippocampal atrophy, contrast with the normal imaging typically seen in delirium unless an underlying structural lesion is present.
One practical example involves an 82-year-old hospitalized for pneumonia who suddenly becomes disoriented and agitated at night. This acute change, combined with inattention and sleep-wake cycle disruption, points strongly to delirium rather than progression of underlying dementia. Delirium can occur in patients with pre-existing dementia, complicating diagnosis, but the superimposed acute decline in function serves as a key indicator. Tools like the Confusion Assessment Method (CAM) help identify the core features: acute onset, inattention, disorganized thinking, and altered level of consciousness. Recognizing this distinction prevents misattribution of symptoms to dementia alone and ensures timely investigation of reversible causes, such as infection, medication side effects, or electrolyte imbalances.
Clinical Classifications of Delirium and Subtypes
Delirium manifests in distinct clinical subtypes, each defined by observable behavioral patterns and psychomotor disturbances. The primary classifications include hyperactive, hypoactive, mixed, and emergence delirium, with agitated delirium and axited delirium representing subforms within the hyperactive spectrum. Patients with hyperactive presentations often display restlessness, rapid speech, and disorientation, while those with hypoactive delirium may appear withdrawn, lethargic, and slow to respond. Emergence delirium occurs specifically during recovery from anesthesia, commonly in pediatric or elderly populations. Assume that
| Subtype | Key Features |
|---|---|
| Agitated delirium | Heightened arousal, aggression, pulling at lines, insomnia |
| Axited delirium | Extreme agitation, autonomic instability, risk of sudden collapse |
| Hypoactive delirium | Reduced motor activity, drowsiness, apathy, slowed thinking |
| Emergence delirium | Confusion post-anesthesia, hallucinations, disorientation |
- Agitated delirium involves marked psychological distress and physical restlessness
- Axited delirium is associated with intense motor agitation and potential cardiovascular strain
- Hypoactive delirium is frequently underdiagnosed due to subtle presentation
- Emergence delirium typically resolves within hours but requires close monitoring
 Hyperactive states: Agitated and Axited delirium
Hyperactive states: Agitated and Axited delirium
 Hyperactive states: Agitated and Axited delirium
Hyperactive states: Agitated and Axited deliriumHyperactive delirium encompasses both agitated and axited subtypes, characterized by elevated motor activity and emotional lability. Agitated delirium presents with pacing, shouting, and resistance to care, often complicating hospital stays in intensive care units. Axited delirium, though less commonly documented, describes a more extreme variant involving profound agitation, diaphoresis, and tachycardia, sometimes progressing to metabolic exhaustion. These states increase the risk of self-extubation, falls, and unplanned removal of catheters. Management typically involves environmental calming, low-dose antipsychotics, and addressing underlying triggers such as infection or medication side effects. A mid-sized SaaS firm managing hospital telemetry data noted increased nurse call alerts during night shifts correlated with undetected agitated episodes.
Hypoactive variants and post-operative emergence delirium
Hypoactive delirium is marked by reduced alertness, minimal verbal output, and slowed movement, often mistaken for depression or sedation. This subtype is particularly prevalent among older adults recovering from surgery or systemic illness, with studies suggesting it accounts for up to 25% of delirium cases in medical wards. Emergence delirium arises during the immediate post-anesthetic period, typically within 30 minutes of waking, and is more common in children receiving sevoflurane or adults with preexisting cognitive vulnerability. Symptoms include thrashing, inconsolable crying, and disorientation despite full arousal. Unlike persistent delirium, emergence episodes usually resolve spontaneously within 10 to 30 minutes. Monitoring protocols in ambulatory surgery centers now include standardized recovery scales to detect these transient but disruptive events.
Recognition of hypoactive and emergence forms remains inconsistent across clinical settings, partly due to their transient or subtle nature. A patient may appear calm yet be profoundly disoriented, delaying intervention. Post-operative protocols at major academic hospitals now integrate routine CAM-ICU screenings during recovery to capture non-agitated cases. Assume that early identification reduces complications and shortens hospital stays.
Alcohol-Related Delirium and Complications
The progression of alcohol withdrawal delirium
Alcohol withdrawal delirium typically emerges 48 to 96 hours after the last drink, marking a severe escalation from earlier withdrawal symptoms such as tremors or anxiety. You may experience sudden confusion, disorientation, and marked agitation, often accompanied by hallucinations that are usually visual or tactile in nature. Without intervention, symptoms can intensify rapidly, with fluctuations in mental status occurring throughout the day, a hallmark of delirium’s acute onset and variable course.
Autonomic instability becomes increasingly evident as the condition progresses, with elevated heart rate, hypertension, and profuse sweating signaling a hyperadrenergic state. You remain at high risk for seizures during this phase, particularly in the first 48 hours, though delirium itself tends to manifest later. A mid-sized SaaS firm’s medical director once reported a case where an employee with untreated alcohol dependence required ICU admission after developing severe confusion and tachycardia following a weekend of abstinence.
Duration varies, but untreated episodes may last up to five days, with mortality rates historically cited in older case series as high as 5% when complications like aspiration or arrhythmias occur. You are more likely to experience prolonged symptoms if prior withdrawal episodes included seizures or cognitive disturbances. Early recognition of this trajectory significantly reduces adverse outcomes.
Identifying and managing delirium tremens (DTs)
Delirium tremens (DTs) is the most severe form of alcohol withdrawal delirium, characterized by profound confusion, hallucinations, and autonomic hyperactivity, typically emerging three to five days after cessation of heavy, prolonged drinking. You may observe extreme agitation, fever, and tachycardia, with some patients exhibiting transient perceptual disturbances such as seeing insects on the skin. DTs affect approximately 5% of individuals undergoing alcohol withdrawal, though incidence varies across clinical settings.
Management hinges on prompt benzodiazepine administration, with lorazepam or diazepam used to control agitation and prevent seizures. You require continuous monitoring in an intensive care environment due to risks of respiratory compromise and cardiac arrhythmias. Thiamine supplementation is administered routinely to prevent Wernicke-Korsakoff syndrome, a neurological complication linked to thiamine deficiency in chronic alcohol users.
Antipsychotics are used cautiously, if at all, due to lowered seizure thresholds; benzodiazepines remain the cornerstone of therapy. You benefit from fluid and electrolyte correction, as dehydration and hypomagnesemia are common. In one documented case at a tertiary hospital, a 52-year-old man with a decade-long history of alcohol dependence stabilized within 72 hours using high-dose diazepam titrated to symptom control.
Recovery from delirium tremens often requires several days of intensive care, with some patients needing prolonged observation to prevent relapse into withdrawal symptoms. You may experience residual cognitive deficits even after resolution, particularly if multiple withdrawal episodes have occurred. Long-term outcomes improve significantly when detoxification is followed by structured addiction treatment and psychosocial support, reducing the likelihood of recurrence.
Identifying Key Clinical Symptoms
Acute cognitive disturbances and disorientation
Confusion in delirium typically emerges over hours to days, distinguishing it from the slower progression of dementia. You may observe sudden difficulty recalling recent events, following conversations, or recognizing familiar surroundings. A patient might not remember the date, location, or even the names of close family members, reflecting a pronounced deficit in orientation. Language impairments such as rambling speech, trouble finding words, or incoherent sentences are common. In one documented case, a 72-year-old hospitalized after hip surgery began misidentifying hospital staff as intruders and insisted he was at home despite clear evidence otherwise. These cognitive disruptions are not static; they evolve rapidly within a single day, often worsening in the evening, a phenomenon known as “sundowning.” Immediate recognition of these signs allows for timely intervention before complications escalate.
Fluctuating levels of awareness and behavioral changes
Attention deficits in delirium can shift dramatically between alertness and near-unresponsiveness. You might notice a patient who was engaged in conversation suddenly staring blankly, unable to respond to simple commands. Some individuals become hyperactive, displaying agitation, restlessness, or even hallucinations—such as seeing insects crawling on walls. Others exhibit hypoactive symptoms, appearing withdrawn, lethargic, or unusually quiet, which can be mistaken for depression. A 68-year-old woman recovering from pneumonia, for example, alternated between pulling at her IV lines and lying motionless for hours. These fluctuations often follow no predictable pattern, making consistent monitoring vital. Behavioral symptoms may include shouting, resisting care, or attempting to get out of bed unassisted, increasing fall risk.
Episodes of altered awareness can last minutes to hours and vary in intensity throughout the day. You may find that a patient responds appropriately during morning rounds but cannot follow instructions by late afternoon. This variability is a hallmark of delirium and differentiates it from other cognitive disorders. Hypoactive forms are frequently underdiagnosed because the symptoms mimic sedation or fatigue. In surgical units, up to 50% of delirium cases are missed without structured screening tools like the Confusion Assessment Method (CAM). Behavioral changes often correlate with underlying physiological stressors such as infection, medication side effects, or metabolic imbalances. Recognizing these patterns enables earlier treatment of root causes and reduces hospital complications.
Management Strategies for Delirium and Therapeutic Options
Conventional clinical interventions and protocols for delirium
Early identification and prompt intervention form the foundation of effective delirium treatment in hospital settings. Standard protocols emphasize correcting underlying causes such as infections, metabolic imbalances, or medication side effects, particularly anticholinergics or benzodiazepines. Non-pharmacological strategies are prioritized, including reorientation techniques, sleep hygiene, mobility assistance, and ensuring the use of hearing aids or glasses when needed. For agitated patients posing a risk to themselves or others, low-dose antipsychotics like haloperidol may be used short-term, though evidence of efficacy remains limited and risks include extrapyramidal symptoms. Multidisciplinary teams in geriatric care units often implement the Hospital Elder Life Program (HELP), which has demonstrated reduced delirium incidence through structured cognitive and physical engagement. These clinical frameworks rely on consistent monitoring using tools like the Confusion Assessment Method (CAM) to track symptom progression and response to treatment.
Pharmacological approaches remain secondary to environmental and supportive care, with benzodiazepines generally avoided except in alcohol or benzodiazepine withdrawal-related delirium. In intensive care units, the ABCDEF bundle—assessing pain, both spontaneous awakening and breathing trials, sedation choice, delirium screening, and early mobility—has become a standard of care. This protocol has been associated with shorter mechanical ventilation duration and reduced delirium prevalence among critically ill patients. Clinicians also review all medications upon admission to eliminate deliriogenic drugs, a step shown to decrease symptom burden within 48 hours in a significant number of cases. These evidence-based interventions reflect a shift toward proactive, preventive models rather than reactive management.
Successful outcomes depend on sustained interdisciplinary coordination, especially in older adults with multiple comorbidities. Nurses play a central role in daily screening and maintaining patient orientation through consistent staffing and personalized care routines. In postoperative settings, protocols that include pre-admission cognitive assessment and intraoperative monitoring of depth of anesthesia have reduced delirium rates in elective surgeries. Hospitals adopting electronic health record alerts for high-risk patients have seen improvements in early intervention timing. These structured clinical responses underscore the importance of system-wide implementation rather than isolated treatments, ensuring that delirium treatment is integrated into routine care pathways across specialties.
Alternative approaches to delirium management: Natural treatments and hypnosis
Some patients and caregivers explore delirium’s natural treatment options, particularly when conventional methods are limited or contraindicated. Herbal supplements such as lemon balm, valerian root, or melatonin are sometimes used to support sleep regulation and reduce agitation, though clinical evidence remains sparse and interactions with prescribed medications must be carefully evaluated. A mid-sized SaaS firm supporting integrative medicine platforms has reported increased user interest in non-pharmacological sleep aids among family members of hospitalized elders. These natural treatments are not substitutes for medical evaluation but may complement environmental strategies like noise reduction and daylight exposure. Essential oils like lavender are occasionally used in aromatherapy protocols within palliative care units, though rigorous studies on their impact on delirium symptoms are lacking.
Hypnosis for delirium is an emerging area of interest, particularly in preoperative and palliative contexts where anxiety and confusion are prevalent. While not a standalone treatment, clinical hypnosis has been applied to reduce pre-surgical stress, which may lower postoperative delirium risk in vulnerable populations. A small pilot study at a teaching hospital in 2022 examined guided hypnosis sessions before cardiac surgery, reporting shorter orientation recovery times in the intervention group. Hypnosis techniques focus on calming imagery, breath regulation, and suggestion-based relaxation, administered by trained therapists. These sessions are typically brief and adapted to cognitive capacity, avoiding complex narratives. Though research is preliminary, the low risk profile of hypnosis makes it a candidate for adjunctive use in multimodal prevention strategies.
Integrating alternative approaches requires careful coordination with medical teams to avoid addressing reversible causes. Natural treatments lack standardized dosing and regulatory oversight, increasing the potential for adverse effects or herb-drug interactions. For instance, St. John’s wort, sometimes used for mood support, can interfere with anticoagulants and antipsychotics commonly prescribed in delirium care. Hypnosis for delirium remains experimental and is not recommended during acute episodes with severe disorientation. However, in subacute or recovery phases, guided relaxation techniques may support cognitive reintegration. These methods are most effective when embedded within a broader care plan that prioritizes safety, medical stability, and evidence-based practices. A growing number of integrative neurology clinics now include trained hypnotherapists as part of dementia and delirium support teams.
Hypnotherapy for Delirium
-
- Attention Deficits: Trance states require sustained focus. Delirious patients typically have severe disturbances in attention and awareness, making standard hypnotic induction impossible. [1, 2, 3, 4]
- Safety & Psychosis Guidelines: In clinical and medical environments, hypnotherapy is generally contraindicated for patients experiencing acute psychosis, severe mental illness, or postoperative delirium because it may worsen these conditions.
- Communication Barriers: Because clear communication and the ability to process goals and instructions are prerequisites for hypnosis, a patient must be oriented and mentally clear to participate safely.
- Dementia Support: Hypnotherapy has been shown to be feasible and acceptable for managing distress, anxiety, and improving daily motivation and socialization in patients with mild-to-moderate dementia.
- Palliative Care: Integrative hypnosis is safely used in supportive care to lower anxiety, reduce fear of falling, and promote relaxation in hospital settings.
- Caregiver Burnout: Caregivers of patients with severe cognitive issues experience high levels of stress. Hypnotherapy is often used to help caregivers manage anxiety and improve their own well-being.
Acupuncture for Delirium Management
-
- Shorter Duration: A randomized controlled trial published in the Journal of Geriatric Psychiatry Neurology showed that older adults receiving daily acupuncture had a significantly shorter time-to-first delirium remission and spent more days delirium-free compared to standard care alone. [, 2]
- ICU Delirium Reduction: A recent clinical trial on critically ill ICU patients noted that those receiving press tack needle acupuncture experienced a significantly higher median number of delirium-free days. [1]
- Surgical Prevention: Systematic reviews confirm that preoperative and intraoperative acupuncture can lower the incidence of postoperative delirium (POD) in elderly individuals undergoing major surgeries.
-
- Attenuating Neuroinflammation: By activating the vagus nerve and cholinergic anti-inflammatory pathways, acupuncture dampens systemic inflammation that often triggers brain dysfunction.
- Neurotransmitter Balancing: It helps stabilize brain chemical levels, including serotonin and norepinephrine, supporting better sleep-wake cycles and cognitive recovery.
- Pain & Medication Management: Acupuncture serves as a low-risk analgesic technique. Reducing physical pain minimizes the clinical requirement for sedatives and opioids, which are primary pharmaceutical triggers of delirium.
-
- Traditional Manual Acupuncture: Ultra-fine needles are inserted into targeted body points like Baihui (GV20) and Yintang (Ex-HN3) to calm the central nervous system.
- Press Tack & Auricular Acupuncture: Small stickers containing tiny, superficial needles are placed on the body or outer ear (specifically the Shenmen point). These can remain in place longer to continuously manage agitation and aggression without disrupting ICU monitoring.
- Transcutaneous Electrical Acupoint Stimulation (TEAS): A non-invasive approach that passes a mild electrical current across the skin’s surface at specific acupoints to achieve anti-inflammatory benefits without using needles.
Homeopathic treatment and management for an acutely disturbed state of mind
-
- Belladonna: Used when delirium is characterized by sudden onset, high fever, intense agitation, and flushed, hot skin with dilated pupils. The patient may appear terrified, seeing monsters or vivid visions, and might try to strike, bite, or escape.
- Stramonium: Indicated for acute, violent, and raging delirium. The patient is typically terrified in the dark, experiences vivid, terrifying hallucinations, and may exhibit loquacity (incessant, rapid talking, laughing, or praying).
- Hyoscyamus niger: Best suited for muttering, low-grade delirium without the extreme violence. The patient is highly suspicious, experiences visual hallucinations (e.g., seeing ghosts or being pursued), and may exhibit involuntary muscle twitching, pick at bedclothes, or try to escape unseen dangers.
- Arsenicum album: Frequently noted in case studies for alcohol withdrawal delirium tremens (DTs) and acute anxiety. It is considered when the delirium is accompanied by extreme physical exhaustion, agonizing restlessness, constant pacing, and severe fear of death.
Conclusion
Delirium arises from a complex interplay of physiological disturbances, medication effects, and underlying conditions such as infection, metabolic imbalance, or substance withdrawal. You may observe its onset acutely in hospitalized patients, particularly among older adults or those in intensive care, where fluctuating mental status, inattention, and disorganized thinking form the core clinical picture. A patient experiencing alcohol-related delirium, for example, might present with agitation, hallucinations, and autonomic instability following abrupt cessation after prolonged use.
Treatment requires identifying and addressing the primary etiology, whether correcting hypoxia, treating sepsis, or adjusting neuroleptic dosing in psychotic features. Non-pharmacological strategies, including reorientation, sleep hygiene, and early mobilization, reduce duration and complications when implemented early. In cases linked to anticholinergic toxicity, discontinuation of the offending agent often leads to rapid improvement.
Outcomes depend on timely recognition and multidisciplinary intervention. You are more likely to see resolution within days to weeks if contributing factors are managed promptly, though persistent cognitive deficits may occur, especially after prolonged episodes. A mid-sized SaaS firm’s health initiative tracking postoperative delirium noted improved recovery times when structured protocols were applied consistently across surgical units.
FAQ

Q: What is delirium, and how is it clinically defined?
A: Delirium is an acute, fluctuating disturbance in attention, awareness, and cognition that develops over a short period, typically hours to days. It is formally defined by diagnostic criteria in the DSM-5 as a disturbance in attention and awareness that is not better explained by another neurocognitive disorder and that represents a change from baseline mental function. The condition is often triggered by an underlying medical condition, substance intoxication or withdrawal, or exposure to a toxin. A patient experiencing delirium may have difficulty focusing on tasks, following conversations, or maintaining coherent thought patterns, with symptoms that tend to vary throughout the day.
Q: How does delirium differ from dementia?
A: Delirium and dementia are distinct clinical entities despite some overlapping symptoms such as confusion and memory impairment. Delirium arises suddenly, often within hours or days, and is typically reversible when the underlying cause is treated. In contrast, dementia develops gradually over months or years and involves progressive, irreversible cognitive decline. A patient with Alzheimer’s disease, for example, may have stable but impaired cognition, whereas someone with delirium may be alert one hour and disoriented the next. Coexistence of both conditions is possible, particularly in older adults, which can complicate diagnosis and management.
Q: What are the primary subtypes of delirium?
A: Delirium is categorized into three main clinical subtypes based on psychomotor behavior: hyperactive, hypoactive, and mixed. Hyperactive delirium is characterized by agitation, restlessness, hallucinations, and combative behavior, often seen during alcohol withdrawal or in intensive care settings. Hypoactive delirium presents with lethargy, slowed movement, drowsiness, and reduced verbal output, frequently mistaken for depression or sedation. Mixed delirium involves alternating periods of hyperactive and hypoactive symptoms. Recognizing the subtype is crucial for appropriate intervention, as hypoactive delirium is often underdiagnosed despite its high prevalence in hospitalized older adults.
A: Delirium tremens (DTs) is a severe form of alcohol withdrawal syndrome that typically occurs 48 to 72 hours after the last drink in individuals with a history of chronic heavy alcohol use. It is marked by profound confusion, autonomic instability (such as tachycardia and hypertension), hallucinations (often visual or tactile), and seizures. DTs represent a medical emergency with significant mortality risk if untreated. It differs from milder forms of alcohol withdrawal delirium by the intensity and duration of symptoms, requiring immediate hospitalization and treatment with benzodiazepines and supportive care.
Q: Can delirium occur after surgery or anesthesia?
A: Yes, postoperative delirium is a common complication, particularly in older adults undergoing major surgeries such as cardiac, orthopedic, or abdominal procedures. It typically emerges within the first few days after surgery and may be triggered by factors including anesthesia exposure, pain, sleep disruption, electrolyte imbalances, or infection. A patient undergoing hip replacement surgery, for instance, may become acutely confused on the second postoperative day, unable to recognize family members or follow simple commands. Incidence rates vary widely depending on the population and surgical type, but it is a recognized contributor to prolonged hospital stays and increased risk of institutionalization.
Q: What are the main treatment strategies for delirium?
A: Treatment focuses on identifying and managing the underlying cause, such as treating infection, correcting metabolic imbalances, or discontinuing offending medications. Non-pharmacological interventions are first-line and include reorientation techniques, maintaining a calm environment, ensuring adequate sleep-wake cycles, and involving family members. Pharmacologic treatment, such as low-dose antipsychotics like haloperidol, may be used cautiously in cases of severe agitation that pose a safety risk. Benzodiazepines are generally avoided except in alcohol or benzodiazepine withdrawal. A multidisciplinary approach involving nurses, physicians, and therapists improves outcomes in hospitalized patients.
Q: Are there any natural or non-drug approaches that help manage an acutely disturbed state of mind?
A: Non-drug strategies form the cornerstone of delirium prevention and management. These include early mobilization, ensuring proper hydration and nutrition, using hearing aids or glasses to reduce sensory deprivation, and minimizing the use of physical restraints or catheters. Some hospitals implement multicomponent programs like the Hospital Elder Life Program (HELP), which uses trained volunteers to engage patients in cognitive stimulation and range-of-motion exercises. While hypnosis and other complementary
A holistic psychiatrist near me
Are you looking for holistic treatment for mental health? Do you or someone you love or care about suffer from ADHD, anxiety, depression, phobias, bipolar, etc.? Google for a holistic psychiatrist near me and find the Philadelphia Holistic Clinic, Philadelphia’s #1 natural treatment facility.
Contact us at (267) 403-3085 to schedule your first visit and discuss your treatment plan and options with Dr. Tsan.