Duodenal Ulcer
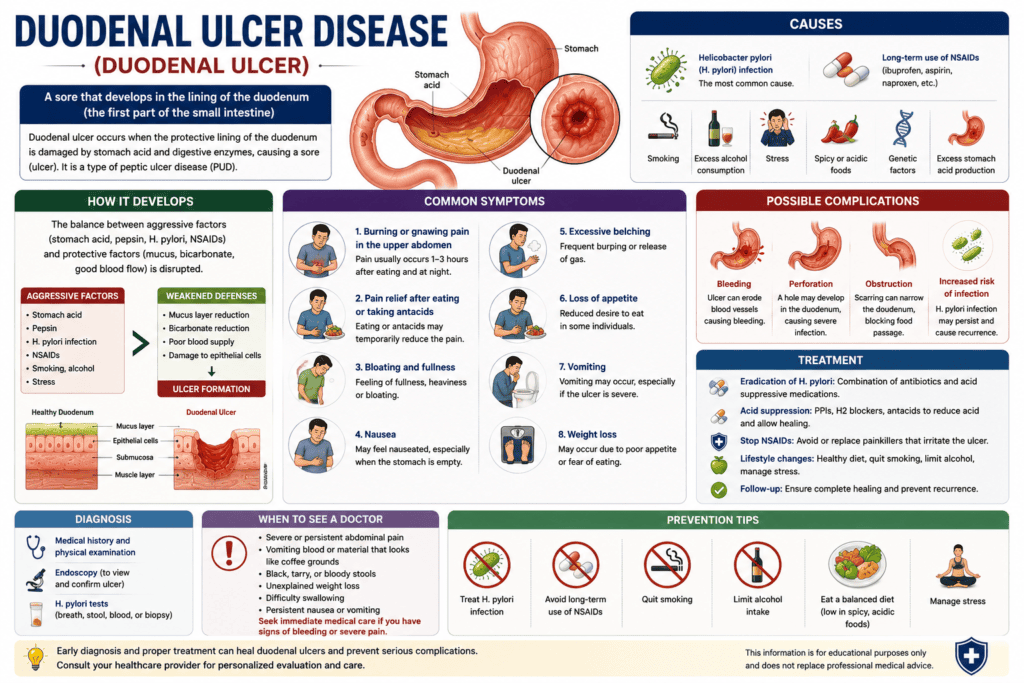
With a gnawing pain in your upper abdomen, you might be experiencing a duodenal ulcer, a common type of peptic ulcer. These open sores form in the lining of the duodenum, the first part of your small intestine. Understanding their origins, recognizing the signs, and exploring comprehensive treatment options are important steps toward recovery. Duodenal ulcer disease involves open sores in the upper section of the small intestine. Caused primarily by H. pylori bacteria or NSAID pain relievers, it triggers burning abdominal pain that worsens on an empty stomach and improves with food or antacids. Treatment includes antibiotics and acid-reducing medications.
Key Takeaways:
- Helicobacter pylori (H. pylori) infection remains the predominant cause of duodenal ulcers, accounting for a significant majority of diagnosed cases.
- Non-steroidal anti-inflammatory drugs (NSAIDs), including common over-the-counter pain relievers, represent the second leading cause of duodenal ulcer formation due to their impact on the protective mucosal lining.
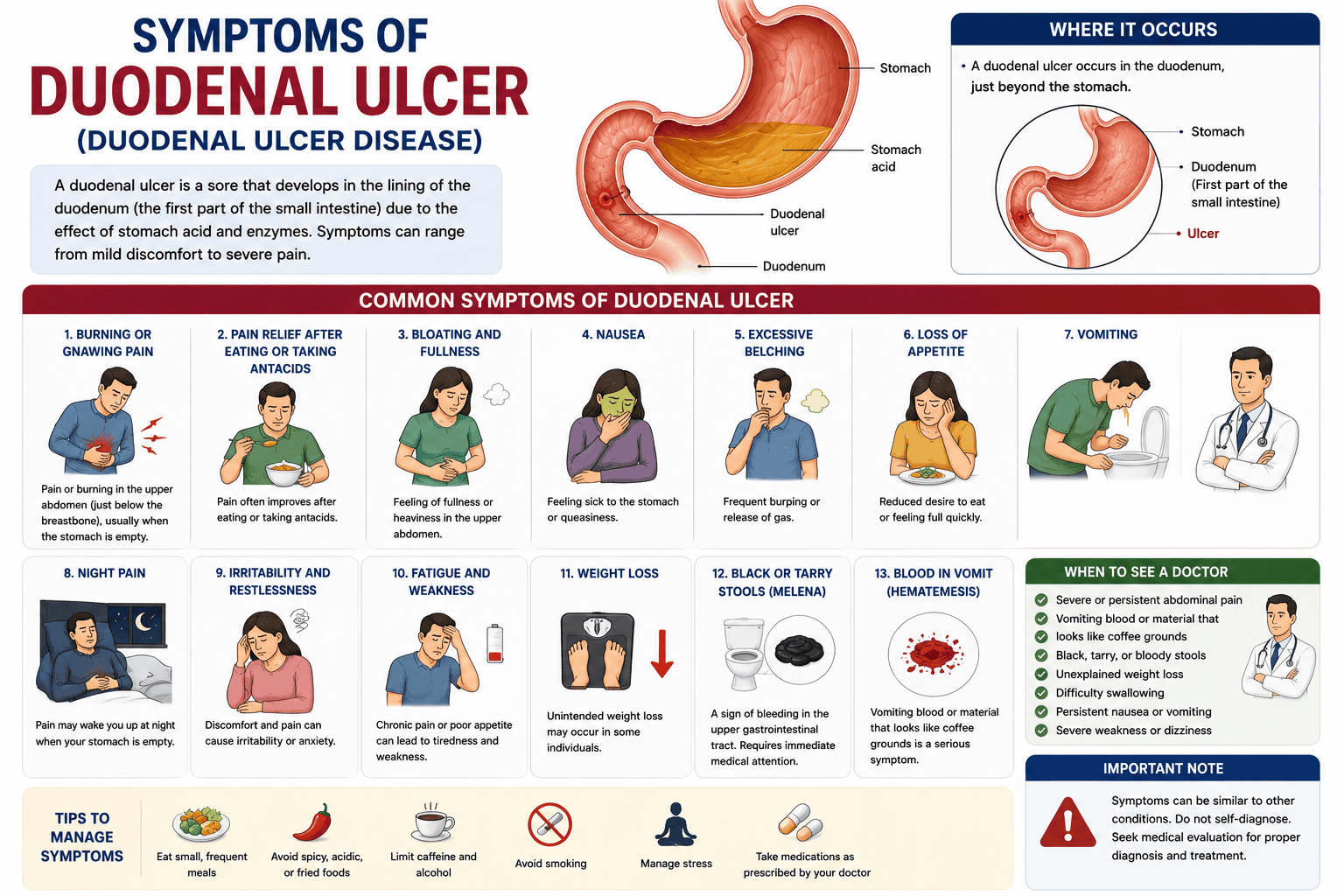
- Burning or gnawing pain in the upper abdomen, often relieved by food or antacids and recurring several hours after eating, is the most characteristic symptom of a duodenal ulcer.
- Distinguishing duodenal ulcers from gastric ulcers is important because gastric ulcer pain typically worsens with food, whereas duodenal ulcer pain often improves with it.
- Conventional treatment for duodenal ulcers primarily involves proton pump inhibitors (PPIs) to reduce acid production and antibiotics to eradicate H. pylori infection when present.
- Dietary modifications, such as avoiding spicy foods, caffeine, and alcohol, can help manage symptoms and support healing, though they do not directly cure the underlying cause of duodenal ulcers.
- Holistic approaches, including stress reduction techniques like mindfulness or yoga, and certain herbal remedies (e.g., deglycyrrhizinated licorice or mastic gum), can complement conventional medical treatments by promoting mucosal integrity and reducing inflammatory responses.
Understanding the Etiology and Pathogenesis of Duodenal Ulcer
Primary biological triggers
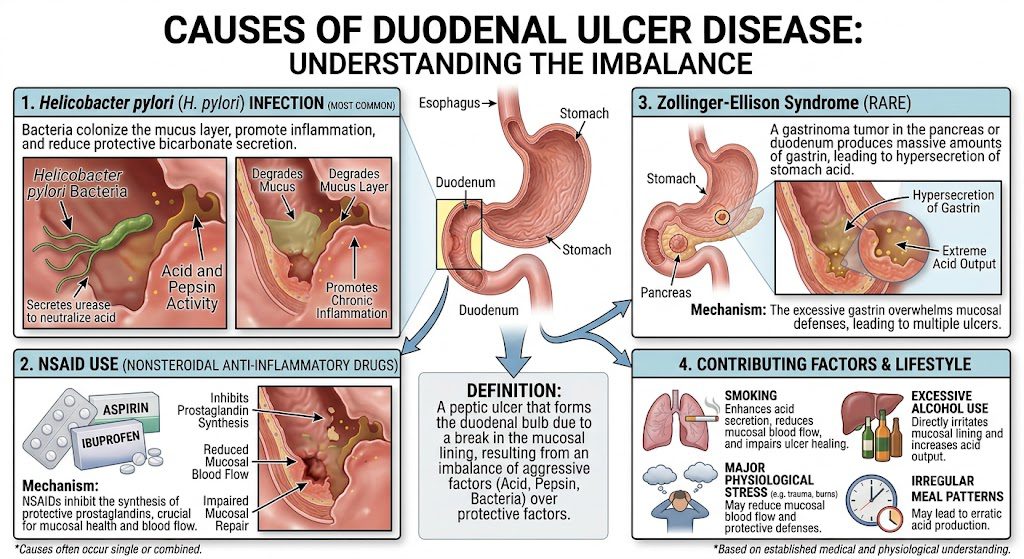
The primary biological trigger for duodenal ulcers is the bacterium *Helicobacter pylori* (*H. pylori*). This Gram-negative bacterium colonizes the stomach lining, leading to chronic inflammation, which in turn increases acid production and weakens the protective mucosal barrier in the duodenum. While not every individual infected with *H. pylori* develops an ulcer, its presence significantly elevates the risk. Another significant factor involves an imbalance between aggressive factors (acid and pepsin) and defensive factors (mucus, bicarbonate, and prostaglandins) in the duodenal lining. When the aggressive forces overwhelm the protective mechanisms, the duodenal mucosa becomes susceptible to erosion and ulcer formation. This delicate balance is critical for maintaining the integrity of the gastrointestinal tract. Genetic predispositions can also play a role in an individual’s susceptibility to duodenal ulcers. Certain genetic variations might influence the immune response to *H. pylori* or affect the production of protective mucosal factors, making some individuals more prone to developing ulcers even with similar exposures to risk factors. A family history of ulcers can often indicate such a predisposition.
Environmental and lifestyle risk factors
Nonsteroidal anti-inflammatory drugs (NSAIDs) represent a major environmental risk factor for duodenal ulcers. Regular use of NSAIDs, such as ibuprofen, naproxen, and aspirin, can damage the duodenal lining by inhibiting prostaglandin synthesis, which is vital to preserving the mucosal barrier and blood flow. This direct chemical irritation makes the duodenum more vulnerable to acid. Smoking significantly increases the risk of developing duodenal ulcers and impedes their healing. Nicotine and other chemicals in cigarette smoke reduce bicarbonate production, decrease blood flow to the duodenum, and accelerate gastric emptying, thereby increasing the acid load on the duodenal bulb. These combined effects contribute to both ulcer formation and persistence. Chronic stress, while not a direct cause, can exacerbate existing conditions and potentially contribute to ulcer development. Stress can alter gastric motility and acid secretion, and it may also impair the immune response, making the body less effective at fighting off *H. pylori* or repairing mucosal damage.
- NSAID use
- Smoking
- Alcohol consumption
- Psychological stress
- Dietary habits (though less direct)
Recognizing these modifiable factors offers clear pathways for prevention and management.
Clinical Presentation and Identification of Duodenal Ulcer
Common physical indicators
Recognizing the common physical indicators of a duodenal ulcer is imperative for timely intervention. You might experience a burning or gnawing pain, typically localized in the upper abdomen, often described as a hunger-like sensation. This discomfort can sometimes radiate to your back, making it difficult to pinpoint the exact source without further examination. Other noticeable symptoms include bloating and a feeling of fullness, even after consuming only a small amount of food. You may also observe changes in your appetite, potentially leading to unintentional weight loss over time. These subtle shifts in your digestive comfort warrant attention, as they can signal underlying ulceration. Nausea and occasional vomiting can also manifest, particularly if the ulcer leads to some degree of gastric outlet obstruction. You might find yourself experiencing frequent burping or a general sense of indigestion that antacids only temporarily alleviate. Observing these persistent physical signs can help guide you toward a professional medical evaluation.
Pain patterns and symptomatic timing
The pain associated with a duodenal ulcer exhibits distinctive patterns that differentiate it from other gastrointestinal discomforts. Typically, you will notice the pain intensifies when your stomach is empty, often several hours after a meal or in the middle of the night. This hunger-like pain is a hallmark characteristic, frequently waking individuals from sleep. Eating food often provides temporary relief from this discomfort, a phenomenon attributed to the buffering effect of food on stomach acid. However, the pain usually returns within two to three hours as the stomach empties and acid production continues. Understanding this cyclical pattern is key to identifying a potential duodenal ulcer. You might also experience periods where symptoms are more severe, followed by weeks or months of reduced discomfort or even complete remission. This episodic nature of duodenal ulcer pain can sometimes lead to delays in seeking diagnosis, as individuals may attribute the relief to other factors. Always consult a healthcare professional if you notice these recurring patterns. The nocturnal exacerbation of pain, often occurring between midnight and 3 AM, is particularly indicative of a duodenal ulcer. At this time, gastric acid secretion is typically at its peak, and the absence of food in the duodenum leaves the ulcerated lining exposed to these corrosive juices, intensifying the burning sensation. This specific timing helps clinicians differentiate duodenal ulcers from other conditions, such as gastric ulcers, where pain is often aggravated immediately after eating.
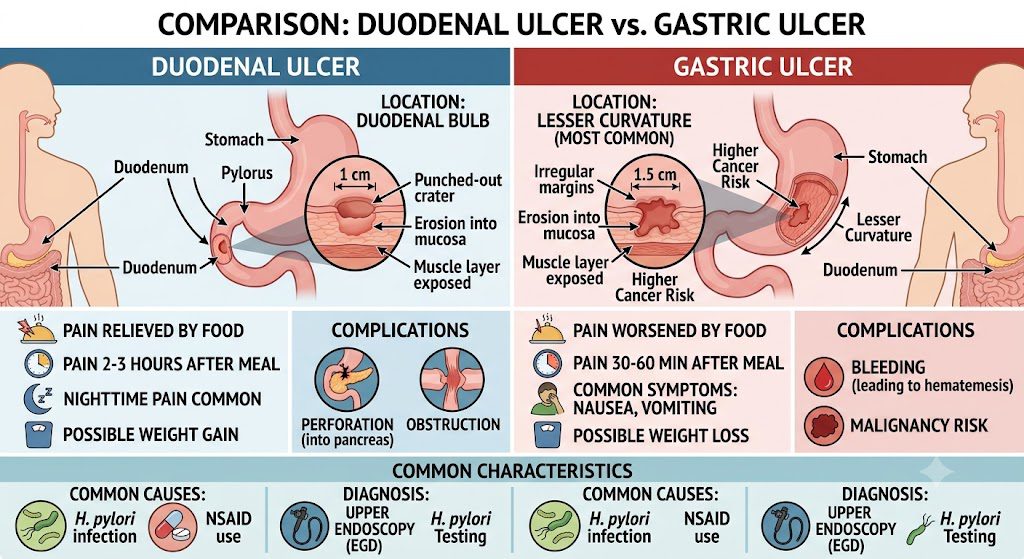
Comparative Analysis: Gastric vs. Duodenal Ulcers
| Gastric Ulcer | Duodenal Ulcer |
|---|---|
| Occur in the stomach lining | Occur in the lining of the duodenum (first part of the small intestine) |
| Pain often worsens with eating (within 30 minutes) | Pain often improves with eating but returns 2-3 hours later |
| Associated with normal or low stomach acid production | Associated with high stomach acid production |
| More common in older adults (over 50) | More common in younger adults (30-50 years old) |
| Higher risk of malignancy | Rarely malignant |
| Weight loss may be present | Weight gain may be present |
| Nausea and vomiting are common | Nausea and vomiting are less common |
| Bleeding is often chronic and occult | Bleeding can be acute and severe (melena or hematemesis) |
 Distinguishing anatomical locations
Distinguishing anatomical locations
 Distinguishing anatomical locations
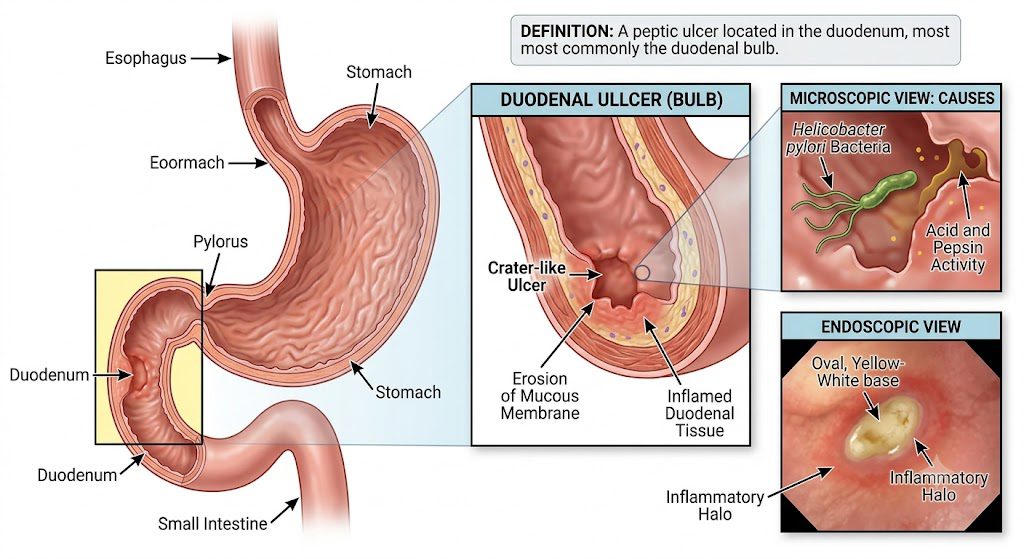
Distinguishing anatomical locationsYou find gastric ulcers forming directly within the stomach’s protective lining. This location means the ulcer is exposed to the direct impact of stomach acid and digestive enzymes immediately after food consumption, often leading to distinct symptomatic patterns. The stomach’s unique environment, designed for initial food breakdown, plays a significant role in how these ulcers present and progress. In contrast, duodenal ulcers develop in the duodenum, specifically the first part of the small intestine, just beyond the stomach’s pyloric sphincter. This segment receives partially digested food and highly acidic chyme from the stomach. The duodenal lining, while resilient, can erode when excessive acid overwhelms its protective mechanisms. Knowing the precise location helps differentiate between the two conditions, guiding diagnostic procedures and treatment strategies. A gastric ulcer, for instance, may require closer monitoring for malignancy, a concern less prevalent with duodenal ulcers, which are rarely malignant. The anatomical distinction underpins the varying clinical presentations you observe.
Variations in symptom triggers and relief
You will notice a key difference in how eating affects the pain associated with each type of ulcer. For gastric ulcers, consuming food often exacerbates the pain, typically within 30 minutes of eating. This response occurs because food stimulates stomach acid production and muscle contractions, directly irritating the ulcerated area in the stomach lining. Conversely, with duodenal ulcers, you may observe that eating actually provides temporary relief from pain. The presence of food in the stomach can dilute stomach acid or trigger the release of bicarbonate, which neutralizes acid as it enters the duodenum. However, this relief is usually transient, with pain returning approximately two to three hours after eating, once the stomach has emptied and acid again bathes the duodenum. Furthermore, gastric ulcers are more commonly associated with symptoms like nausea and vomiting, potentially due to the direct irritation of the stomach lining or impaired gastric emptying. Duodenal ulcers, while causing significant discomfort, typically present with less frequent nausea and vomiting, focusing more on the post-meal pain cycle. You will observe that individuals with gastric ulcers sometimes experience weight loss, possibly because the pain after eating discourages them from consuming adequate food. In contrast, those with duodenal ulcers might even experience weight gain, as eating temporarily alleviates their discomfort, leading to more frequent food intake. Bleeding patterns also differ, with gastric ulcers often exhibiting chronic and occult bleeding, while duodenal ulcers can lead to acute and severe bleeding, sometimes presenting as melena or hematemesis.
Conventional and Integrated Medical Management of Duodenal Ulcer
Standard pharmacological protocols for duodenal ulcer
Pharmacological intervention for duodenal ulcers primarily targets the reduction of gastric acid secretion and the eradication of *Helicobacter pylori* infection when present. Proton pump inhibitors (PPIs) like omeprazole, lansoprazole, and pantoprazole are cornerstones of therapy, effectively suppressing acid production by inhibiting the H+/K+-ATPase pump in gastric parietal cells. You typically take these once daily for four to eight weeks, allowing the ulcer to heal. When an *H. pylori* infection is confirmed, a multi-drug regimen is necessary to eliminate the bacteria. This often involves a combination of a PPI with two antibiotics, such as amoxicillin and clarithromycin, or metronidazole and clarithromycin, administered for 7 to 14 days. This triple therapy approach significantly increases eradication rates, reducing the likelihood of ulcer recurrence. Bismuth quadruple therapy, comprising a PPI, bismuth subsalicylate, tetracycline, and metronidazole, serves as an alternative for cases of treatment failure or clarithromycin resistance. This more intensive regimen is typically prescribed for 10 to 14 days and is highly effective against resistant strains, offering another pathway to successful bacterial eradication and ulcer healing.
Monitoring recovery and preventing recurrence
Monitoring your recovery from a duodenal ulcer involves both symptom assessment and, in some cases, follow-up endoscopic procedures. Your doctor will ask about the resolution of pain, heartburn, and other digestive discomforts, which are key indicators of healing. The absence of symptoms often suggests successful treatment and ulcer closure. Preventing recurrence is a critical aspect of long-term management, especially after successful initial treatment. If *H. pylori* was identified, confirming its eradication is paramount; this is typically done via a urea breath test, stool antigen test, or biopsy several weeks after completing antibiotic therapy. Successful eradication dramatically lowers the risk of future ulcers. You should also address lifestyle factors that contribute to ulcer formation or hinder healing. This includes avoiding non-steroidal anti-inflammatory drugs (NSAIDs) if possible, reducing alcohol consumption, and quitting smoking, all of which can irritate the duodenal lining and impede recovery. Managing stress through various techniques also plays a supportive role in preventing future episodes.
Nutritional Strategies and Dietary Interventions for Duodenal Ulcer
Adopting specific nutritional strategies is fundamental for managing duodenal ulcers, offering a supportive role alongside medical treatments. Focusing on foods that reduce inflammation and promote mucosal healing can significantly alleviate symptoms and contribute to long-term recovery. Your dietary choices directly influence the gastric environment, making informed decisions paramount for therapeutic success. You will find that certain foods can exacerbate symptoms, while others provide protective benefits to the duodenal lining. Understanding this distinction allows you to tailor your diet effectively, minimizing irritation and supporting the body’s natural healing processes. This personalized approach to nutrition is a cornerstone of holistic ulcer management. Implementing a well-structured dietary plan can also help address potential nutritional deficiencies that may arise from altered digestion or absorption due to the ulcer. By prioritizing nutrient-dense foods, you ensure your body receives the necessary building blocks for tissue repair and overall health, reinforcing your body’s resilience against future ulcer recurrence.
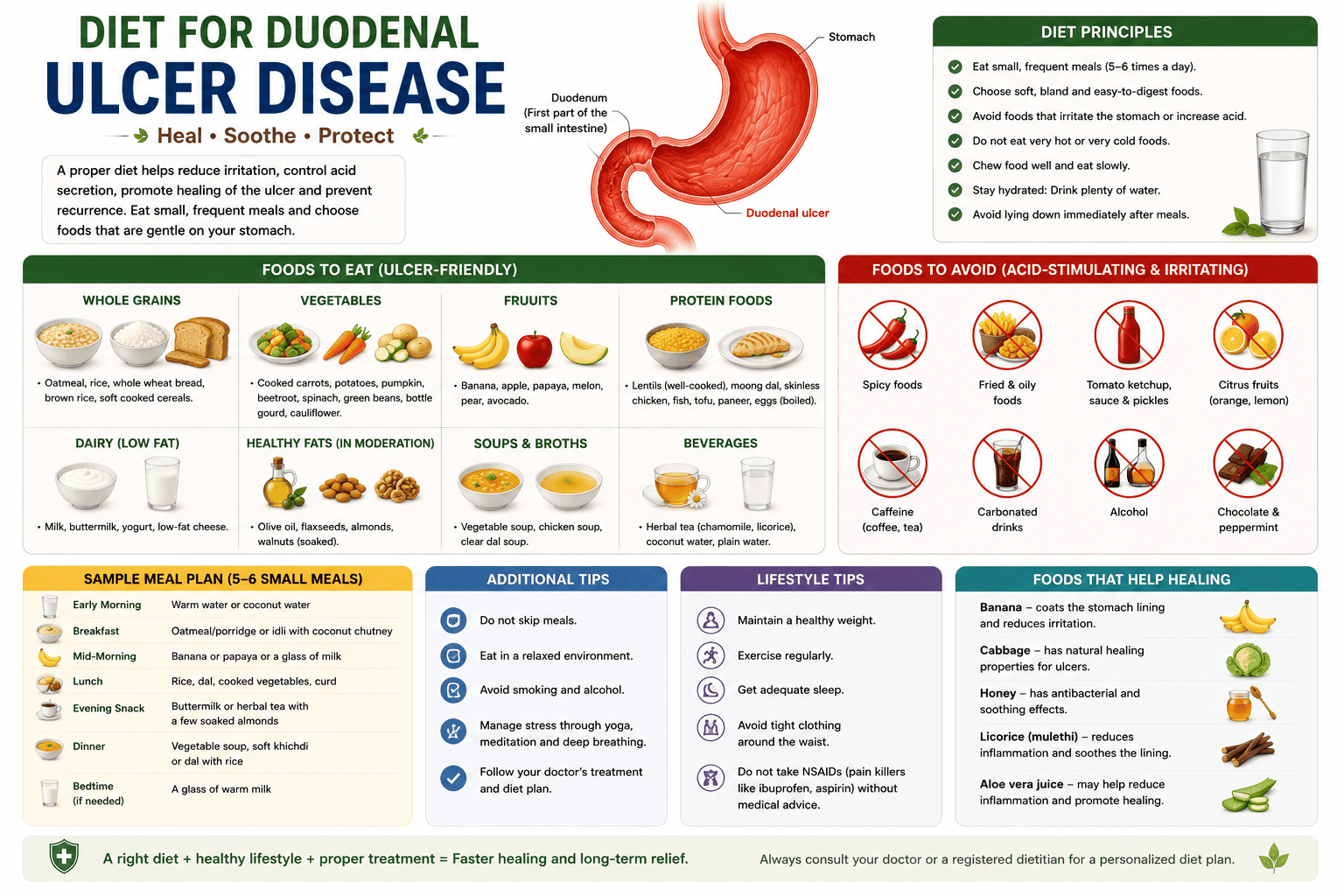
Recommended food groups for mucosal healing
Focus on incorporating foods rich in antioxidants and anti-inflammatory compounds to aid in mucosal repair. Berries, leafy greens, and colorful vegetables, for instance, provide a wide spectrum of vitamins and phytochemicals that support cellular regeneration and reduce oxidative stress in the duodenal lining. These foods also contribute important fiber, which can help regulate digestion. Lean proteins are also crucial for tissue repair, supplying the amino acids necessary for rebuilding damaged cells. Including sources like fish, poultry, and legumes ensures a steady supply of these building blocks without introducing excessive fats that might delay gastric emptying or increase acid production. Aim for moderate portions at each meal to support continuous healing. Healthy fats, such as those found in avocados, olive oil, and flaxseeds, contribute to cell membrane integrity and can have anti-inflammatory effects. These fats also assist in the absorption of fat-soluble vitamins (A, D, E, K), which play various roles in immune function and tissue maintenance, further supporting your recovery.
Identifying and eliminating dietary irritants
Identifying and subsequently removing dietary irritants is a critical step in alleviating duodenal ulcer symptoms and promoting healing. Common culprits often include spicy foods, which can directly irritate the ulcerated mucosa, and highly acidic items like citrus fruits and tomatoes, which may increase gastric acid levels. Keeping a detailed food diary can help pinpoint your specific triggers. Caffeine and alcohol are significant irritants; both can stimulate acid production, leading to increased pain and delayed healing. Reducing or completely eliminating these beverages, even temporarily, can provide substantial relief and create a more favorable environment for the duodenal lining to recover. Pay attention to hidden sources of caffeine, such as certain teas and chocolates. Processed foods, often high in unhealthy fats, sugar, and artificial additives, can also contribute to inflammation and digestive distress. These items lack the beneficial nutrients found in whole foods and can place additional stress on your digestive system, hindering the healing process. Prioritizing whole, unprocessed foods is always a better choice for your overall health. You might discover that even seemingly innocuous foods can cause discomfort for you, given the individual nature of ulcer sensitivity. For example, some individuals find that dairy products or gluten-containing grains exacerbate their symptoms, even though these are not universal irritants. A systematic approach to eliminating and reintroducing foods, perhaps under the guidance of a healthcare professional, can help you precisely identify your personal dietary triggers.
Holistic and Complementary Approaches to Duodenal Ulcer Treatment
Evidence-based natural healing modalities for duodenal ulcer
Natural treatments for duodenal ulcers often focus on supporting the body’s healing processes and reducing inflammation. You might consider specific herbal remedies, for example, which have been historically utilized to soothe the digestive tract and promote mucosal integrity. For instance, licorice root (deglycyrrhizinated licorice or DGL) is frequently recommended for its ability to increase mucus production, forming a protective barrier against stomach acid. Other botanical interventions include mastic gum, derived from the mastic tree, which has shown promise in inhibiting *Helicobacter pylori* (H. pylori) bacteria, a common contributor to duodenal ulcers. Certain studies suggest that even specific forms of cabbage juice, rich in glutamine, can accelerate ulcer healing by providing crucial nutrients for gut lining repair. These natural compounds offer a less invasive pathway to managing ulcer symptoms and promoting recovery. You can also explore the benefits of aloe vera, known for its anti-inflammatory and wound-healing properties. Consuming pure aloe vera juice (ensure it’s food-grade and free of aloin, a laxative compound) may help calm an irritated duodenal lining. Furthermore, incorporating probiotics, found in fermented foods or supplements, can help restore a healthy gut microbiome, which is crucial for overall digestive health and can indirectly support ulcer healing.
Integration of traditional and homeopathic therapies for duodenal ulcer
Acupuncture for duodenal ulcer treatment offers a complementary avenue for pain management and digestive regulation. This ancient practice involves the precise insertion of thin needles into specific points on the body, aiming to rebalance the body’s energy flow (Qi) and stimulate natural healing mechanisms. Patients often report reduced ulcer pain and improved digestive function following a course of acupuncture sessions. Homeopathic remedies for duodenal ulcer conditions are individualized, meaning a practitioner selects a remedy based on your specific symptoms, constitution, and overall health picture. Common homeopathic substances used for ulcer symptoms might include *Nux vomica* for indigestion and irritability or *Arsenicum album* for burning pains and anxiety, though the choice is always highly personalized to the patient’s unique presentation. These highly diluted preparations aim to stimulate the body’s innate healing response. Integrating these traditional and homeopathic approaches into your treatment plan can provide a multi-faceted strategy for managing duodenal ulcers. This might involve continuing conventional medical treatments while simultaneously undergoing acupuncture to alleviate pain and stress or consulting with a homeopath for a tailored remedy to address underlying imbalances. The goal is to support your body’s recovery through various well-established, patient-centered modalities.
Homeopathic Claims and Context
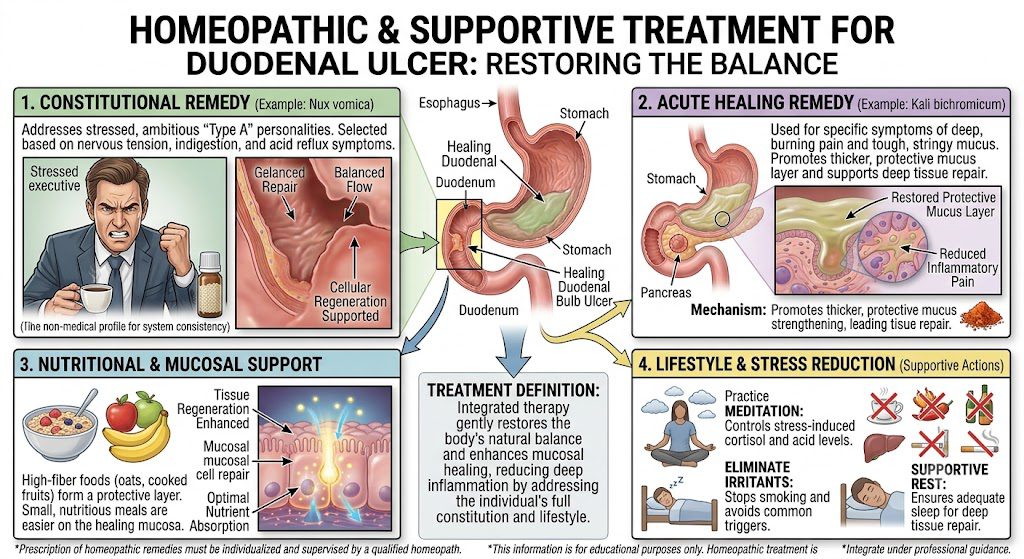
- Nux vomica: Often selected by homeopaths for digestive discomfort, cramping, or “hunger pains” that worsen on an empty stomach.
- Sulphur or Lycopodium: Used in alternating or sequential protocols depending on the practitioner’s assessment of changing symptoms.
- Carbo vegetabilis: Mentioned in alternative text sources for accompanying bloating or burning distress.
Conclusion
You have gained an understanding of duodenal ulcers, from their primary causes, like *H. pylori* infection and NSAID use, to the characteristic symptoms such as epigastric pain and bloating. Recognizing these indicators early allows for timely intervention, mitigating the potential for more severe complications. A comprehensive approach to managing this condition integrates conventional medical treatments with supportive lifestyle adjustments, offering you a clearer path toward recovery. Addressing the underlying factors is paramount in your journey to healing. You can achieve successful outcomes by eradicating *H. pylori* with appropriate antibiotic regimens and by modifying or discontinuing NSAID use where feasible. Incorporating dietary changes, such as identifying and avoiding trigger foods while increasing intake of protective nutrients, significantly contributes to mucosal healing and symptom reduction. These combined efforts create a more resilient digestive environment for you. Your commitment to a holistic recovery path, encompassing stress management techniques and consistent adherence to medical advice, plays a pivotal role in preventing recurrence. By prioritizing your digestive health through informed choices and proactive management, you can effectively manage duodenal ulcers and improve your overall well-being.
FAQ

Q: What are the primary causes of duodenal ulcers?
A: The most common cause of duodenal ulcers is infection with the bacterium Helicobacter pylori (H. pylori). This bacterium can colonize the stomach lining and duodenum, leading to inflammation and erosion. Another significant contributor is the regular use of non-steroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen or naproxen, which can irritate the duodenal lining and impair its natural protective mechanisms. Zollinger-Ellison syndrome, a rare condition causing excessive acid production, can also lead to duodenal ulcer formation.
Q: How do the symptoms of a duodenal ulcer typically manifest?
- Abdominal Pain: A dull or burning sensation in the upper abdomen, typically between your breastbone and belly button.
- Pain Relief with Food: Unlike stomach ulcers, duodenal ulcer pain usually gets worse 1 to 3 hours after a meal when the stomach empties and is temporarily alleviated by eating or antacids.
- Nighttime Pain: The pain is notorious for occurring early in the morning or waking you up in the middle of the night.
- Digestive Distress: Bloating, frequent belching, and a feeling of excess fullness after a small meal.
Q: How does a duodenal ulcer differ from a gastric ulcer?
A: While both are types of peptic ulcers, their locations and symptom patterns often differ. A duodenal ulcer occurs in the duodenum, the first part of the small intestine, whereas a gastric ulcer forms in the stomach lining. Pain from a duodenal ulcer typically improves with food, only to return later, often several hours after eating. Gastric ulcer pain, conversely, may be exacerbated by eating. Duodenal ulcers are also more common than gastric ulcers, representing about 80% of all peptic ulcers.
Q: What are some conventional medical treatments for duodenal ulcers?
A: Conventional medical treatment usually involves a combination of medications. Proton pump inhibitors (PPIs), such as omeprazole or lansoprazole, reduce stomach acid production, allowing the ulcer to heal. H2-receptor blockers, like famotidine, also decrease acid secretion. If H. pylori is present, a course of antibiotics is prescribed, often a combination of two or three different drugs, along with a PPI, to eradicate the infection. Bismuth subsalicylate is sometimes included in eradication regimens.
Q: Can dietary changes help manage duodenal ulcer symptoms?
A: While specific foods do not cause or cure duodenal ulcers, certain dietary adjustments can help manage symptoms and support healing. Avoiding foods that trigger increased acid production or irritation, such as spicy foods, acidic fruits, caffeine, and alcohol, can be beneficial. Eating smaller, more frequent meals can prevent excessive stomach distension and acid surges. Incorporating fiber-rich foods, lean proteins, and healthy fats can support overall digestive health and mucosal integrity.
Q: What holistic approaches are considered for duodenal ulcers?
A: Holistic approaches aim to support the body’s healing processes and reduce contributing factors. Stress reduction techniques, including meditation, yoga, and deep breathing exercises, can be helpful, as stress can exacerbate ulcer symptoms. Herbal remedies like deglycyrrhizinated licorice (DGL) or mastic gum are sometimes used to protect the mucosal lining and inhibit H. pylori growth. Acupuncture may also be explored for pain management and to promote digestive balance. Probiotics, found in fermented foods or supplements, can support gut flora balance, especially after antibiotic treatment.
Q: Are there any specific natural remedies or supplements often recommended for duodenal ulcers?
A: Several natural remedies and supplements are explored for their potential benefits in managing duodenal ulcers. Mastic gum, derived from the mastic tree, has demonstrated antimicrobial properties against H. pylori in some studies. Deglycyrrhizinated licorice (DGL) is thought to stimulate the production of protective mucus in the stomach and duodenum. Aloe vera juice, known for its soothing properties, may help reduce inflammation. Zinc carnosine is another supplement sometimes used to support the integrity of the gastrointestinal lining and accelerate ulcer healing. Always consult a healthcare professional before integrating supplements into a treatment plan.
Holistic Treatment for Duodenal Ulcer Disease in Philadelphia
If you decide to treat your duodenal ulcer naturally, you have many possibilities. The value offered by the majority of the solutions mentioned above will impress you; all you need to do is figure out which one works for you. In addition to being incredibly healthful, they will protect your stomach and naturally treat any ulcer symptoms. Avoid utilizing excessive amounts of any chemical, as even these cures for duodenal ulcers can cause problems if used excessively. To avoid any negative interactions with your present therapies, speaking with a medical professional is crucial. These natural remedies are amazing and effective for the majority of people, so give them a try!
Philadelphia Holistic Clinic, the home of holistic medicine in Philadelphia, sits in the northeast of the City of Brotherly Love. The clinic quickly became the metro area’s leading acupuncture, homeopathy, and hypnotherapy center. Dr. Tsan, the clinic’s medical director, has over 40 years of academic and practical experience in internal medicine and naturopathy.
Victor Tsan, MD, an internationally recognized specialist in traditional Chinese medicine, classical homeopathy, and clinical hypnotherapy, graduated from the most famous medical schools in Europe, Asia, and the USA.
For your initial holistic evaluation by Victor Tsan, MD, contact our clinic at (267) 403-3085 or book it online.